Radiation Oncology/CNS/Acoustic neuroma
< Radiation Oncology < CNS
|
Epidemiology
The overall incidence of symptomatic acoustic neuromas is 1/100,000 persons, however, autopsy results have shown that subclinical acoustic neuromas are present in up to 1% of people. Acoustic neuromas account for ~8% of intracranial tumors and 80-90% of CPA tumors. Most people with symptomatic acoustic neuromas will present between the ages of 30 and 50. They are almost always unilateral; bilateral acoustic neuromas are limited to patients with NF-2.
Risk Factors
- Acoustic trauma: OR of 2.2 if 10 years exposure to extremely loud noise, OR of 13.1 if 20 or more years of exposure.
- Parathyroid adenoma: OR of 3.4 for acoustic neuromas.
- NF-2: Accounts for 10% of patients with acoustic neuroma, typically bilateral. Recall that NF2 gene is a tumor suppressor gene on chromosome 22 that encodes a membrane cytoskeletal protein called merlin or schwannomin that appears to be involved in actin-cytoskeleton organization. NF2 associated with bilateral ANs, gliomas, meningiomas, cataracts, and neurofibromas.
Pathology
Acoustic neuromas arise from the Schwann cell perineural elements of the affected nerve and occur with equal frequency on the superior and inferior branches of the vestibular nerve (rarely affect the cochlear portion of CN VIII). They arise at the junction of the central myelin produced by glial cells and peripheral myelin produced by Schwann cells (Obersteiner-Redlich zone). On light microscopy one will see zones of alternately dense and sparse cellularity called Antoni A and B areas, respectively. Acoustic neuromas will also stain positive for the S100 protein.
Natural History
The natural history of acoustic neuromas is variable. The average growth rate is 1.9mm/year. 40% of tumors overall (higher for smaller tumors) will show no growth or even shrinkage on serial images. However, there is no predictive relation between growth rate and size of tumor at presentation.
Clinical Presentation
The symptoms involved with acoustic neuroma are due to cranial nerve involvement and tumor progression.
- Acoustic nerve: Symptomatic involvement in 95% of patients, major symptoms being hearing loss and tinnitus. Hearing loss present in 95%, but only about 66% were actually aware of this deficit. The hearing loss is usually chronic (over years). Tinnitus is present in 63% of patients.
- Vestibular nerve: Involved in 61% of patients and manifests as mild to moderate unsteadiness while walking. True spinning vertigo is uncommon due to the slow growing nature of these tumors.
- Trigeminal nerve: Disturbance occurs in 17% of patients with symptoms such as facial numbness, hypesthesia, and pain. These symptoms usually occur after hearing loss is present for more than two years, and vestibular symptoms for more than one year.
- Facial nerve: Involved in 6% of patients. Seen as facial paresis and taste disturbances.
- Posterior fossa: Compression on the cerebellum or brainstem results in ataxia. May also see serious complications such as brainstem compression, cerebellar tonsillar herniation, hydrocephalus, and death.
Work-up
- Physical Exam:
- Confirm sensorineural hearing loss with Rinne test (tuning fork on mastoid bone, AC>BC) and Weber test (vibratory sound louder on the “good” side)
- Also check for other CN deficits (absent corneal reflex, facial twitching, hypesthesia)
- Audiometry:
- The best initial screening test
- Typically shows asymmetric SHL, usually more prominent in the higher frequencies. Functional hearing typically described as <50 dB and >50% speech discrimination
- Hearing loss does not necessarily correlate with tumor size.
- Brainstem auditory evoked potentials: Delay in conduction time on the affected side.
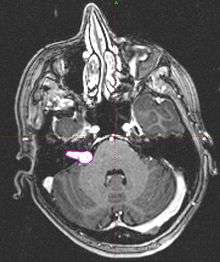
- Imaging: MRI with gadolinium can detect tumors as small as 1-2mm. Seen as an enhancing lesion “ice cream cone” in the region of internal acoustic canal or a “dumbbell” extending into the foramen magnum.
Treatment
The three treatment options for acoustic neuroma are surgery, radiation therapy, and observation.
Surgery
Typically performed by an otologist and a neurosurgeon. The learning curve is very steep, on the order of 20-60 cases. There are three surgical approaches used in the removal of acoustic neuromas.
- Retromastoid suboccipital: An incision is made behind the ear and the mastoid bone and some inner ear structures are removed. Advantages to this approach include decreased risk of facial nerve damage and ability to attempt hearing preservation. A disadvantage is that using this approach, if the tumor extends distally into the IAC, complete removal may not be possible.
- Middle fossa: This approach involves an incision just anterior to the ear with removal of the underlying bone to expose the area of interest. Hearing preservation is attempted with this approach, but depending on location of the tumor complete removal may not be feasible.
- Translabyrinthine: This approach goes directly through the inner ear and invariably sacrifices hearing.
Results: Anatomic preservation of the facial nerve is achieved in 93% of patients and of the cochlear nerve in 68%. Hearing preservation rate for surgery is 47%. Complications of surgery: Death (1%), hemiparesis (1%), CN palsey (5%), hematomas (2.2%), CSF fistulas (9.2%), hydrocephalus (2.3%), bacterial meningitis (1.2%), wound revisions (1.1%). (Samii, Neurosurgery 1997 Jan;40(1):11-21)
Radiosurgery
GKS--Patient’s head is fixed in MRI compatible Leksell stereotactic frame and 1-1.5mm slice MRI is obtained. Prescribe dose of 12.5-13.0 Gy to the 50% isodose line. TV defined as macroscopic tumor seen on MRI/CT. Evaluate dose fall-off to cochlea and brain stem. Tumor control rate (97%), Normal facial function (>99%), Trigeminal function (97%), Hearing preservation (up to 77%). (Lunsford, J Neurosurg 2005 Jan;102 Suppl:195-9)
Proton Beam Radiosurgery--Now only used for pts with non-serviceable hearing and tumors <2.0cm. Use 3 fiducial markers in the outer table of the cranium, as well as placement of head in a stereotactic frame. A 3D CT based planning system is used. 160 MeV proton beam is used to administer 3 converging beams to a max dose of 13 cobalt Gray equivalents to TV. Evaluate dose fall-off to brainstem and cochlea. Excellent tumor control (95%) and preservation of CNs V (89%) and VII (91%) Hearing preservation: 33%. (Weber, Neurosurgery 2003 Sep;53(3):577-86)
Fractionated stereotactic radiotherapy--Patient’s head is immobilized in a mask and linear accelerator is used to apply the radiation. Dose: 50-55 Gy in 25-30 fractions to the 80% isodose line. The data for FSR has shown excellent tumor control, preservation of hearing/CN function, and reduced treatment related toxicity. (Combs, IJROBP 2005 Sep 1; 63 (1):75-81)
Observation
In certain cases it may be feasible to observe the patient and his/her VS with MRI scans every 6-12 months. Problems with this approach include ongoing hearing loss, and possible mass effects with large tumors.
External Beam RT
- Thomas Jefferson; 2009 PMID 19042095 -- "Toward dose optimization for fractionated stereotactic radiotherapy for acoustic neuromas: comparison of two dose cohorts." (Andrews DW, Int J Radiat Oncol Biol Phys. 2009 Jun 1;74(2):419-26. Epub 2008 Nov 29.)
- Retrospective. 89 patients. Two dose levels: 50.4 Gy vs 46.8 Gy. Median F/U 4.4 and 5.4 years
- Outcome: Tumor control 100% both groups.
- Toxicity: Raw 3-year hearing preservation 46.8 Gy 79% vs. 50.4 Gy 68% (SS). Pure tone hearing better in low-dose cohort 46.8 Gy 33db vs. 50.4 Gy 40 db (SS). Actuarial hearing preservation rate significantly longer for low-dose group 3.2 years vs. 1.5 years (SS). Predictors for hearing dose cohort and pretreatment hearing class
- Conclusion: Lower dose of 46.8 Gy had 100% local control with better hearing preservation rate
- Harvard; 2005 (1992-2001) PMID 15987541 -- "Stereotactic radiotherapy for vestibular schwannomas: favorable outcome with minimal toxicity." (Chan AW, Neurosurgery. 2005 Jul;57(1):60-70; discussion 60-70.)
- Retrospective. 70 patients (new 47%, progressive after observation 31%, postop 3%, recurrent 19%), NF2 in 11 patients. Treated with linac SRT. Median dose 54/30 to 95% isodose. Median tumor volume 2.4 cm3. Median F/U 3.8 years
- Outcome: 3-year LC 100%, 5-year LC 98%. Freedom from resection 98% and 92%. Initial tumor volume predictive of resection: 5-year FFR if <8 cm3 97% vs. >8 cm3 47%. No difference due to NF2 status
- Toxicity: 3-year facial nerve 99%, trigeminal nerve 96%. Prior surgery predictive of TN toxicity (86% vs. 98%)
- Conclusion: Conventionally fractionated SRT results in very favorable outcome
Comparison of radiosurgery and surgery
- France, 2002 - PMID 12450031 — "Functional outcome after gamma knife surgery or microsurgery for vestibular schwannomas." Regis et al.,J Neurosurgery. 2002 Nov;97(5):1091-100.
- Non-randomized prospective series using pre- and post-operative questionnaires to evaluate functional outcomes after GKS or microsurgery. The minimum follow-up was 3 years, the GKS group had 97 patients and the microsurgery group had 110 patients. Outcomes in table below:
| Facial motor disturbance | CN V disturbance | Preserved Hearing | Overall functional disturbance | Hospital Stay (Days) | Mean days missed from work | ||
| Surgery | 37% | 29% | 37.5% | 39% | 23 | 130 | |
| GKS | 0% | 4% | 70% | 9% | 3 | 7 |
- Baylor, 2002 (1993-2000) - PMID 12459364 — "Treatment of acoustic neuroma: stereotactic radiosurgery vs. microsurgery." Karpinos M et al. Int J Radiat Oncol Biol Phys. 2002 Dec 1;54(5):1410-21.
- Retrospective. 75 pts with Gamma Knife, 25 with microsurgery.
- No difference in tumor control. RS more effective in: preservation of measurable hearing (57% vs 14%). Microsurgery had higher rate of: facial neuropathy (35%/6%) and trigeminal neuropathy (22%/12%). Also no difference in: serviceable hearing, tinnitus, imbalance, dysarthria, dysphagia, and headache. Longer hospital stay and more perioperative complications (47% vs 4%) for microsurgery.
Comparison of SRS and FSRT
- Amsterdam; 2003 PMID 12873685 -- "Single-fraction vs. fractionated linac-based stereotactic radiosurgery for vestibular schwannoma: a single-institution study." (Meijer OW, IJROBP. 2003 Aug 1;56(5):1390-6). 129 patients with ANs from 1992-1999 were prospectively selected for SRS or FSRT based on whether or not they had teeth. All treatments were linac based. The dentate patients received FSRT (20Gy/5fx and 25Gy/5fx) and the edentate patients received SRS (10Gy and 12.5Gy). Mean follow-up was 33 months. Results in table below.
| Tumor Control | CN V preservation | CN VII Perservation | Hearing Preservation | ||
| SRS | 100% | 92% | 93% | 75% | |
| FSRT | 94% | 98% | 97% | 61% |
- Conclusion: Comparable rate of tumor control and preservation of hearing, CN V, and CN VII.
- Thomas Jefferson; 2001 (1994-2000) PMID 11483338 -- "Stereotactic radiosurgery and fractionated stereotactic radiotherapy for the treatment of acoustic schwannomas: comparative observations of 125 patients treated at one institution." (Andrews, IJROBP. 2001 Aug 1;50(5):1265-78).
- Retrospective. 122 patients (GKS 69, fractionated 52). GKS dose 12 Gy, fractionated dose 50/25. Mean F/U 2.3 years
- Outcome: tumor control SRS 98% vs. FSRT 97% (NS)
- Toxicity: CN V preservation 95% vs. 93% (NS), CN VII preservation 98% vs. 98% (NS); functional hearing 33% vs. 81% (SS)
- Conclusions: Comparable rates of tumor control and CN preservation, improvement in servicable hearing
Proton Therapy
- Harvard; 2003 (1992-2000) PMID 12943574 -- "Proton beam radiosurgery for vestibular schwannoma: tumor control and cranial nerve toxicity." (Weber DC, Neurosurgery. 2003 Sep;53(3):577-86; discussion 586-8.)
- Retrospective. 88 patients, proton SRS. Median volume 1.4 cm3. Prior surgery 17%. Facial nerve function normal 90%, good/excellent hearing 9%, servicable hearing 15%. Median dose 12 CGE (10-18 CGE) prescribed to median 70% isodose line. Median F/U 3.2 years
- Outcome: 5-year LC 94%, radiological reduction in 95%
- Toxicity: In GR Grade 1-2, 33% retained servicable (GR Grade 2) hearing. 5-year normal facial nerve 91% and trigeminal nerve 89%. Facial neuropathy predicted by prescribed dose, maximum dose, and inhomogeneity
- Conclusion: Proton beam SRS effective treatment, reduced prescribed dose associated with decrease in facial neuropathy
- Loma Linda; 2002 (1991-1999) PMID 11844261 -- "Fractionated proton beam radiotherapy for acoustic neuroma." (Bush DA, Neurosurgery. 2002 Feb;50(2):270-3; discussion 273-5.)
- Retrospective. 31 ANs in 30 patients. Mean tumor volume 4.3 cm3. If useful hearing, 54 CGE, if no hearing 60 CGE. Mean F/U 2.8 years
- Outcome: 0% progression, 38% regression
- Toxicity: 31% maintained useful hearing. No CNV or CNVII dysfunction
- Outcome: Fractionated PT excellent LC
Toxicity
- Please see Inner Ear NTCP for more information
Bevacizumab
- Harvard; 2009 PMID 19587327 -- "Hearing improvement after bevacizumab in patients with neurofibromatosis type 2." (Plotkin SR, N Engl J Med. 2009 Jul 23;361(4):358-67. Epub 2009 Jul 8.)
- Retrospective. 10 patients, NF-2 and progressive vestibular schwannoma, not candidates for surgery/RT. Treated with bevacizumab 5 mg/kg, median duration of therapy 12 months
- Outcome: tumor shrinkage in 9/10; best volumetric reduction 26%. Hearing response 4/7, stable 2/7, progressive hearing loss 1/7
- Conclusion: VEGF blockade improved hearing in some patients, and was associated with volume reduction