Adult pulseless arrest
Immediate
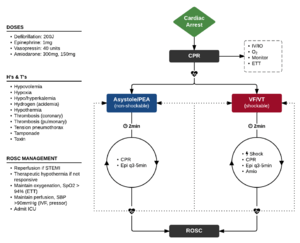
Algorithm for cardiac arrest (Adapted from ACLS 2010)
- Start CPR
- Give oxygen
- Attach monitor/defibrilator
- Rhythm shockable?
V-Fib and Pulseless V-Tach (Shockable)
- Shock as quickly as possible and resume CPR immediately after shocking
- Biphasic - 200J
- Monophasic - 360 J
- Give Epi 1mg if (shock + 2min of CPR) fails to convert the rhythm
- Give antiarrhythmic if (2nd shock + 2min of CPR) again fails
- 1st line: Amiodarone 300mg IVP with repeat dose of 150mg as indicated
- 2nd line: Lidocaine 1-1.5mg/kg then 0.5-0.75mg/kg q5-10min
- Polymorphic V-tach: Magnesium 2g IV, followed by maintenance infusion
Asystole and PEA (Non-Shockable)
- Epi 1mg q3-5min
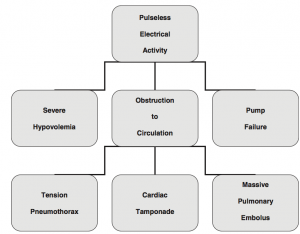
- Three major mechanisms of PEA (3 & 3 Rule)
- Severe Hypovolemia
- Obstruction
- Pump Failure
Treatable ACLS Conditions (H's and T's)
- Hypovolemia
- Hypoxemia
- Hydrogen ion (i.e. acidemia)
- Hypo/hyperkalemia
- Hypothermia
- Tension Pneumothorax
- Cardiac tamponade
- Toxins
- Thrombosis, pulmonary
- Thrombosis, coronary
PEA Evaluation by QRS
Differential based on QRS being narrow or wide and aided by ultrasound
QRS Narrow
Mechanical RV Problem – Ultrasound should show hyperdynamic LV and potential cause
QRS Widened
Metabolic LV Problem – Ultrasound should show hypokinetic LV
- Severe hyperkalemia
- Sodium-channel blocker toxicity (Ex. Tricyclic (TCA) toxicity)
- Agonal rhythm
- Acute MI with pump failure
General
- A (adjunct) - Place oropharyngeal airway
- B (breathing) - place on Ventilator to assure slow ventilation rate (attach to BVM mask)
- 10-12 bpm, 500cc tidal volume, Fio2 100%
- C (compressions) - Switch out providers q pulse check; use metronome
- D - defibrillation
- May be ok to shock during compressions if wearing gloves and using biphasic device[1]
- Precharge prior to pulse & rhythm check to increase overall compression time
- A (advanced airway)
- Use LMA (NOT ET tube - no break in compressions required)
- B (advanced breathing)
- Connect LMA to Ventilator
- Pressure control 20, RR 10, insp rate 1.5-2s
- Connect LMA to Ventilator
- C (advanced circulation)
- Place IO instead of central line
- D (differential)
Refractory Ventricular Fibrillation
A patient is considered refractory after ≥3 defib, ≥3mg epinephrine, and 300mg amiodarone
The following therapies are largely based on case studies or case series
Dual Sequential Defibrillation[2] [3]
- Continue high quality CPR
- Place a second set of defib pads in an alternative location on the chest (anterior/posterior and right upper chest/left lateral)
- Deliver 200J (or 360J if monophasic) simultaneously from both defibrillators
- Continue CPR
Esmolol for Electrical Storm [4][5][6]
- Administer Esmolol bolus 500 mcg/kg IVP over 30 seconds (typical dose ranges 35-50 mg)
- If ROSC, initiate 50 mcg/kg/min infusion [7]
- Deliver 200J (or 360J if monophasic) simultaneously from both defibrillators
- Continue CPR
Consider holding further epinephrine (The Current State of Refractory VF)
Fibrinolytics
Dosing
- Alteplase 0.6mg/kg IV push x1 given over 15 min (± heparin 5000 unit bolus), and then repeated 30 min after if still no ROSC[8]
- Heparin may be bolused with tPA or after ROSC obtained
- Max doses of 50mg may be as efficacious as 100mg
- Consider at least 20min of CPR after last dose of tPA before ending code
See Also
References
- Lloyd MS, Heeke B, Walter PF, and Langberg JJ. Hands-on defibrillation: an analysis of current flow through rescuers in direct contact with patients during biphasic external defibrillation. Circulation. 2008; 117:2510-2514.
- Hoch DH et al. Double Sequential External Shocks for Refractory Ventricular fibrillation. JACC 1994; 23: 1141 – 5.
- Bero M et al. Changing the management of refractory ventricular fibrillation: the consideration of earlier utilization of dual sequential defibrillation. Am J Emerg Med. 2019 May 29. pii: S0735-6757(19)30359-6. doi: 10.1016
- Driver BE, Debaty G, Plummer DW, et al. Use of esmolol after failure of standard cardiopulmonary resuscitation to treat patients with ventricular fibrillation. Resuscitation. 2014; 85(10):1337-1341.
- Boehm KM. First report of survival in refractory ventricular fibrillation after dual-axis defibrillation and esmolol administration. West J Emerg Med. 2016 Nov;17(6):762-765.
- Lee YH. Refractory ventricular fibrillation treated with esmolol. Resuscitation. 2016 Oct;107:150-5. doi: 10.1016.
- Al-Khatib SM. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac arrest. Circulation. 2018 Sep 25;138(13):e272-e391. doi: 10.1161
- Böttiger BW et al. Lancet 2001;357:1583-5.
- Kearon C et al. Chest 2012; 141 (2)(suppl):e419s-e494s. Vanden Hoek TL et al. Circulation 2010; 122 (suppl):S829-S861.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.