Urolithiasis
Background
Urolithiasis comprises 3 similar clinical entities:
- Nephrolithiasis
- Ureterolithiasis
- Cystolithiasis
The most common cause is infection of residual bladder urine with urea-spliting organisms (proteus, pseudomonas, klebsiella, staphlococcus and mycoplasm)
Renal damage
- Irreversible renal damage can occur within 3 weeks in patients with a complete obstruction
- Most have no rise in creatinine because unobstructed kidney functions at up to 185% of its baseline capacity
Infection
Stone Expulsion Rate
| Stone Size | Passage Rate[2] |
| 1-4 mm | 78% |
| 5 -7 mm | 60% |
| >8mm | 39% |
Types
- Calcium (75%)
- Hyperparathyroidism, hypercalcemia of malignancy, sarcoidosis, increased absorption, loop diuretics, IBD
- Struvite (magnesium-ammonium-phosphate) (15%)
- Uric Acid (10%)
- 25% of patients with gout develop kidney stones
Risk Factors for Complications
- Renal function at risk
- DM
- Hypertension
- Renal insufficiency
- Single kidney
- Horseshoe kidney
- Transplanted kidney
- History of difficulty with stones
- Extractions
- Stents
- Ureterostomy tubes
- Lithotripsy
- Symptoms of infection
Clinical Features
- Pain
- Acute onset, crampy, intermittent, unable to find position of comfort
- Location of pain depends on location of stone:
- Upper ureter: flank pain
- Mid ureter: lower anterior quadrant of abdomen
- Distal ureter: groin pain
- UVJ: Can mimic a UTI (frequency, urgency, dysuria)
- Nausea/vomiting (50%)
- Hematuria (85%)
Differential Diagnosis
Nephrolithiasis is most common misdiagnosis given to patients with rupturing AAA
Flank Pain
- Vascular
- Abdominal aortic aneurysm
- Renal artery embolism
- Renal vein thrombosis
- Aortic dissection
- Mesenteric ischemia
- Renal
- Pyelonephritis
- Papillary necrosis
- Renal cell carcinoma
- Renal infarction
- Renal hemorrhage
- Ureter
- Nephrolithiasis
- Blood clot
- Stricture
- Tumor (primary or metastatic)
- Bladder
- Tumor
- Varicose vein
- Cystitis
- GI
- Biliary colic
- Pancreatitis
- Perforated peptic ulcer
- Appendicitis (appendix may be pushed to RUQ in pregnancy)
- Inguinal Hernia
- Diverticulitis
- Cancer
- Bowel obstruction
- Gynecologic
- GU
- Other
- Shingles
- Lower lobe pneumonia
- Retroperitoneal hematoma/abscess/tumor
- Epidural abscess
- Epidural hematoma
Lower Back Pain
- Spine related
- Acute ligamentous injury
- Acute muscle strain
- Disk herniation (Sciatica)
- Degenerative joint disease
- Spondylolithesis
- Epidural compression syndromes
- Spinal fracture
- Cancer metastasis
- Spinal stenosis
- Transverse myelitis
- Vertebral osteomyelitis
- Ankylosing spondylitis
- Spondylolisthesis
- Discitis
- Renal disease
- Kidney stone
- Pyelonephritis
- Nephrolithiasis
- Intra-abdominal
- Abdominal aortic aneurysm
- Ulcer perforation
- Retrocecal appendicitis
- Large bowel obstruction
- Pancreatitis
- Pelvic disease
- PID
- Other
Evaluation
Labs
- Urinalysis: hematuria
- Urine culture :
- Urine pregnancy
- Chemistry
- CBC: If concern for infection (>15k concerning)
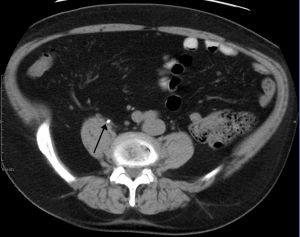
Imaging
- Consider tailoring your choice of imaging based upon the patient's age, clinical likelihood of stones, risk factors, and prior history of stones[4]
- In young patients, even with no prior history of kidney stones, reasonable approaches may be bedside ultrasound or no imaging
- In middle aged patients with prior history of stones, it may be reasonable to perform a bedside ultrasound although no imaging can be appropriate as well
- In middle aged patients with no prior history of stones, CT imaging is reasonable
- In elderly patients, even with prior history of stones, CT is recommended in order to avoid missing alternative etiologies such as dissection, AAA, or diverticulitis.
- Bedside Renal ultrasound

- Consider non-contrast CT abdomen and pelvis (KUB protocol) for:
- 1st time stone
- Older patients with other possible diagnosis
- Avoid CT in young (<50 years old), health patients with known history of nephrolithiasis with presentation consistent with renal colic[5]
- Consider formal ultrasound for:
- Pregnant pt
- Repeat stone (to avoid CT)
- In comparison of diagnosis by CT vs. U/S (by EP) vs. U/S (by radiologist):[6]
- No difference in rate of missed high-risk diagnoses that resulted in complications (pyelo/sepsis/diverticular abscess)
- No difference in rate of serious adverse events, pain scores, return emergency department visits, or hospitalizations
Management
Pain
- Ketorolac 15mg IV or Ibuprofen 600mg PO Q6hrs PRN if the patient can tolerate oral medications[7]
- Avoid high dose NSAIDS in patients with renal failure or insufficiency.
- Ketorolac 15 mg has similar effects to traditional 30 mg dosage. [8]
- Morphine or other Opioids are often needed due to severe pain
Antiemetic
Expulsion Therapy
- Consider Tamsulosin 0.4mg PO QHS (discontinued after successful expulsion; average 1-2 weeks)
- See EBQ:Alpha-blockers for ureteral stone expulsion discussion of evidence
- 76% vs 48% passage rates in tamsulosin vs no treatment, respectively[9]
- Only patients with stones ≥ 5 mm benefited
- Review of 55 RTCs, with NNT of 4
- Tamsulosin number needed to harm (orthostatic hypotension)= 19 (give at night, to reduce side effect rate)[3]
- Use of IV fluids to "flush out" stone has NOT been shown to improve clinical outcomes[3]
Infected Urolithiasis
Inpatient observation is often the safest disposition for patients with infected stones due to the risk of progressing to sepsis. All antibiotics should take into account patient's previous sensitivities and local antibiograms Treatment is targeted at E. coli, Enterococcus, Klebsiella, Proteus mirabilis, S. saprophyticus
Outpatient
Consider one dose of Ceftriaxone 1g IV or Gentamycin 7mg/kg IV if the regional susceptibility of TMP/SMX or Fluoroquinolones is <80%
- Ciprofloxacin 500mg PO BID x7 days OR
- Trimethoprim-Sulfamethoxazole DS 160/800mg PO BID x14 days OR[10]
- Cephalexin 500mg QID PO x 10-14 days (OR consider 1000mg BID if difficulty with QID regimen) OR
- Cefdinir 300mg BID PO x 10-14 days OR
- Cefpodoxime 200mg PO BID x 10 days OR[11]
- Cefixime 400mg PO daily x 10 days OR[12]
- Levofloxacin 750mg PO QD x7 days[13]
Adult Inpatient Options
- Ciprofloxacin 400mg IV q12hr OR
- Ceftriaxone 1gm IV QD OR
- Cefotaxime 1-2gm IV q8hr OR
- Gentamicin 3mg/kg/day divided q8hr +/- ampicillin 1–2 gm q4hr OR
- Piperacillin/Tazobactam 3.375 gm IV q6hr OR
- Cefepime 2gm IV q8hr OR
- Imipenem 500mg IV q8hr
Pediatric Inpatient Options
- Ceftriaxone 75mg/kg IV QD OR
- Cefotaxime 50mg/kg IV q8hrs OR
- Ampicillin 25mg/kg IV q6hrs + Gentamicin 2.5mg/kg IV q8hrs
Surgical Removal
Considered for ureterolithiasis with:
- Persistent obstruction
- Failure of stone progression
- Increasing or unremitting colic
- Staghorn calculi
Disposition
Admission
Recommended for any of the following:
- Intractable pain or vomiting[3]
- Proximal urinary tract infection,[3] as evidence by:
- Urosepsis:
- Fever
- Ill appearance, OR
- Markedly elevated WBC
- Single or transplanted kidney with obstruction[3]
- Acute renal failure[3]
- Hypercalcemic Crisis
Also consider admission for patients with:
- Solitary kidney or transplanted kidney without obstruction
- Urinary extravasation
- Significant medical comorbidities
Consultation
Discharge
- Small stone, adequate analgesia, able to arrange urology follow up within 7d
See Also
References
- Abrahamian FM, et al. Association of pyuria and clinical characteristics with presence of urinary tract infection among patients with acute nephrolithiasis. Annals of EM. 2013; 62(5):526-533.
- Coll DM et al. Relationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. AJR Am J Roentgenol 2002 Jan; 178:101-3.
- Wang RC. Managing Urolithiasis. Annals of EM. April 2016. 67(4):449-454
- Imaging in suspected renal colic: systematic review of the literature and multispecialty consensus Moore CL, Carpenter CR, Heilbrun ME, et al. Ann Emerg Med. 2019;74(3):391-399.
- Part of Choosing wisely ACEP
- Smith-Bindman R, Aubin C, Bailitz J, et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. NEJM. 2014; 371(12):1100–1110.
- Pathan, SA et al. Delivering safe and effective analgesia for management of renal colic in the emergency department: a double-blind, multi-group, randomised controlled trial. Lancet. 2016 May 14;387(10032): 1999-2007
- Motov S, et al. Comparison of Intravenous Ketorolac at Three Single-Dose Regimens for Treating Acute Pain in the Emergency Department: A Randomized Controlled Trial. Ann Emerg Med. 2017 Aug;70(2):177-184. doi: 10.1016
- Hollingsworth JM et al. α-blockers for treatment of ureteric stones: systematic review and meta-analysis. BMJ 2016;355:i6112.
- Gupta K, Hooton TM, Naber KG, et al. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women. Clinical Infectious Diseases. 2011;52(5):e103-e120. doi:10.1093/cid/ciq257
- Colgan R, Williams M. Diagnosis and treatment of acute uncomplicated cystitis. Am Fam Physician. 2011 Oct 1;84(7):771-6.
- Acute Pyelonephritis in Adults. Johnson, JR and Russo, TA. New England Journal of Medicine 2018; 378:48-59.
- Sandberg T. et al. Ciprofloxacin for 7 days versus 14 days in women with acute pyelonephritis: a randomised, open-label and double-blind, placebo-controlled, non-inferiority trial. Lancet. 2012 Aug 4;380(9840):484-90.