Tricuspid atresia
Background
- A cyanotic congenital heart defect
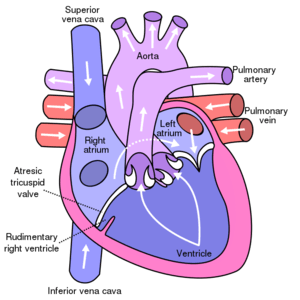
- Absence of tricuspid valve resulting in absence of communication between the right atrium and right ventricle
- Due to absence of communication with the right ventricle, RV becomes either under-developed or entirely absent
- Third most common cyanotic congenital heart disease [1]
Associated cardiac lesions
- ASD (100%)
- Right ventricular hypoplasia (100%)
- VSD (95%)
- Pulmonary outflow obstruction (75%)
- Transposition of the great arteries (28%)
Physiology
- Blood from the RA must exit through the ASD (no tricuspid valve)
- Right to left atrial shunting allows deoxygenated systemic venous blood to enter the LA, then LV
- Cyanosis is present due to mixing of systemic and pulmonary venous blood in the LA
Clinical Features
- 50% present on the first day of life, additional 30% present by 1 month of age
- Central cyanosis is the most notable feature on physical exam and can be progressive
- May also present with poor feeding
- Holosystolic murmur at left lower sternal border if VSD is present
- Continuous murmur if there is a [[PDA
- Jugular venous distention and prominent “a” wave and hepatomegaly if there is a restrictive atrial level communication
- Tachypnea may be present in patients with unrestrictive pulmonary blood flow
- EKG may show left axis deviation and LVH
- Heart size is normal typically
Differential Diagnosis
Congenital Heart Disease Types
- Cyanotic
- Acyanotic
- AV canal defect
- Atrial septal defect (ASD)
- Ventricular septal defect (VSD)
- Cor triatriatum
- Patent ductus arteriosus (PDA)
- Pulmonary/aortic stenosis
- Coarctation of the aorta
- Differentiation by pulmonary vascularity on CXR[2]
- Increased pulmonary vascularity
- Decreased pulmonary vascularity
- Tetralogy of fallot
- Rare heart diseases with pulmonic stenosis
Evaluation
- Echocardiography
- Chest x-ray
- May have a paucity of pulmonary markings and normal heart size in patients with normal pulmonary blood flow (no VSD)
- May have cardiomegaly and prominence of pulmonary vascularity in patients with increased pulmonary blood flow (large VSD)
- ECG
- May demonstrate tall P waves, left axis deviation, LVH, and diminished RV forces
Management
- Stabilize cardiopulmonary function prior to surgery
- Supplemental oxygen
- Mechanical ventilation
- Inotropic agents (eg, dopamine and dobutamine) improve myocardial contractility
- Prostaglandin E1
- Maintain adequate ductal dependent pulmonary flow
- Start infusion at 0.05 mcg/kg/min IV and titrate up to 0.1 mcg/kg/min, monitoring for hypotension and apnea
- Side Effects: Hypotension, Bradycardia, Seizures and Apnea
- Staged surgical repair
Disposition
- Admit
See Also
External Links
References
- Reller MD. Prevalence of congenital heart defects in metropolitan Atlanta, 1998-2005. J Pediatr. 2008;153(6):807-13.
- Knipe K et al. Cyanotic congenital heart diseases. Radiopaedia. http://radiopaedia.org/articles/cyanotic-congenital-heart-disease
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.