Transposition of the great arteries
Background
- Type of cyanotic congenital heart disease
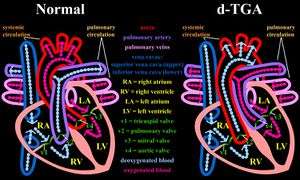
- Aorta arises from the right ventricle and the pulmonary artery from the left ventricle
- Results in two parallel circulations
- The first sends deoxygenated systemic venous blood to the right atrium and back to the systemic circulation via the right ventricle and aorta
- The second sends oxygenated pulmonary venous blood to the left atrium and back to the lungs via the left ventricle and pulmonary artery
- Incompatible with life unless there is communication between the two parallel circuits
- Mixing occurs either intracardiac (patent foramen ovale, VSD or ASD) OR extracardiac connections (patent ductus arteriosus or bronchopulmonary collateral circulation)
- Often associated with other cardiac abnormalities
- Ventricular septal defects (VSD)
- Left ventricular outflow tract obstruction (dynamic or anatomical)
- Mitral and tricuspid valve abnormalities
- Coronary artery variations
- Prevalence in the United States is estimated to be 4.7 per 10,000 live births[1]
- Accounts for 3% of all congenital heart disease and almost 20% of all cyanotic CHD defects [2]
Clinical Features
- Cyanosis, determined by amount of intercirculatory mixing
- Tachypnea
- Murmurs
- Pansystolic murmur at lower left sternal border if there is a VSD
- Systolic ejection murmur along the upper left sternal border in patients with left ventricular outflow obstruction
- Diminished pulses in patients who also have coarctation of the aorta or interruption of the aortic arch
Differential Diagnosis
Congenital Heart Disease Types
- Cyanotic
- Acyanotic
- AV canal defect
- Atrial septal defect (ASD)
- Ventricular septal defect (VSD)
- Cor triatriatum
- Patent ductus arteriosus (PDA)
- Pulmonary/aortic stenosis
- Coarctation of the aorta
- Differentiation by pulmonary vascularity on CXR[3]
- Increased pulmonary vascularity
- Decreased pulmonary vascularity
- Tetralogy of fallot
- Rare heart diseases with pulmonic stenosis
Evaluation
"Egg on side/string" sign
- Echocardiography
- ECG
- Initial ECG often normal
- CXR
- Classically with “egg on a string” appearance, thought to be a result of the great arteries forming a narrowed vascular pedicle when transposed
- Cardiac catheterization
- Remains the gold standard, but seldom required to make the diagnosis
Management
- Stabilization of cardiac and pulmonary function and ensure adequate systemic oxygenation
- Prostaglandin E1
- Provide sufficient intercirculatory mixing between the two parallel circulations by maintaining patency of the ductus arteriosus
- Start infusion at 0.05 mcg/kg/min IV and titrate up to 0.1 mcg/kg/min, monitoring for hypotension (and apnea)
- Maintains the ductus (which completely seals by ~3 wks)
- Side Effects: Hypotension, Bradycardia, Seizures and Apnea
- Balloon atrial septostomy
- Performed to stabilize patients with severe hypoxemia due to inadequate mixing between the two parallel circuits
- Balloon is placed across the atrial septum into the left atrium, inflated and then pulled vigorously back across the septum to produce an ASD
- Surgery, Arterial switch operation
- In rare instances, atrial switch operation when coronary artery anatomy makes arterial switch infeasible
- Typically performed within the first two weeks of life
- Most will die within the first year of life without treatment
Disposition
- Admit
See Also
External Links
References
- Improved national prevalence estimates for 18 selected major birth defects--United States, 1999-2001. MMWR Morb Mortal Wkly Rep. 2006;54(51):1301-5.
- Reller MD. Prevalence of congenital heart defects in metropolitan Atlanta, 1998-2005. J Pediatr. 2008;153(6):807-13.
- Knipe K et al. Cyanotic congenital heart diseases. Radiopaedia. http://radiopaedia.org/articles/cyanotic-congenital-heart-disease
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.