Tracheostomy bleeding
Background
Tracheostomy Sizes
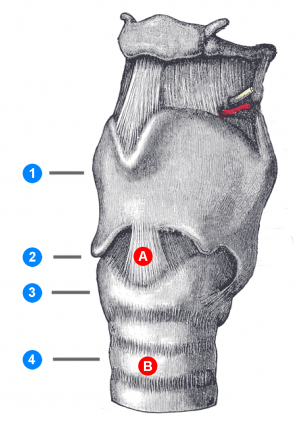
(1) Thyroid cartilage (2) Cricothyroid ligament (3) Cricoid cartilage (4) Trachea (A) Cricothyrotomy site (B) Tracheotomy site
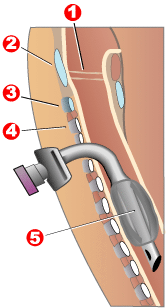
Tracheotomy in situ
1 – Vocal folds
2 – Thyroid cartilage
3 – Cricoid cartilage
4 – Tracheal rings
5 – Balloon cuff
1 – Vocal folds
2 – Thyroid cartilage
3 – Cricoid cartilage
4 – Tracheal rings
5 – Balloon cuff
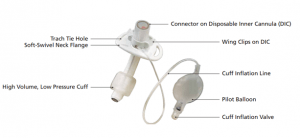
Shiley™ trach tube
- Average size:
- Adult: 5-10mm
- Peds: 2.5-6.5mm
Tracheostomy vs laryngectomy
It is important to differentiate between tracheostomy vs laryngectomy
- If laryngectomy[1]:
- The stoma is the only way to ventilate the patient.
- Patient cannot be orally intubated
Clinical Features
- Minor bleeds within first few days usually due to:
- Lack of hemostasis
- Tube suction and manipulation
- Tracking of blood from nearby surgical site
Risk Factors
- Infection
- Corticosteroids
- Diabetes
Differential Diagnosis
Evaluation
- Large bleed is tracheoinnominate fistula until proven otherwise
Management
- Local Bleeding
- Use silver nitrate if bleeding source is identified
- Brisk Bleeding
- Tracheoinnominate artery fistula (TIF) until proven otherwise
- Most patients present within first 3wk after tracheostomy
- Very high mortality rate
- Delegate team member to obtain surgical assistance, especially with massive bleed
- Treatment:
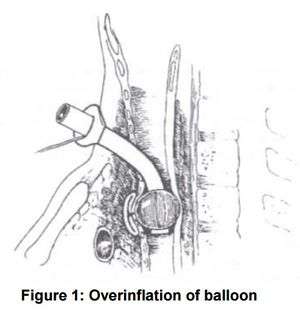
- Hyperinflate the cuff (85% successful), up to 50 cc to tamponade bleeding
- If above fails, withdraw tube while placing pressure against anterior trachea
- ETT from above (as long as there is no laryngectomy)
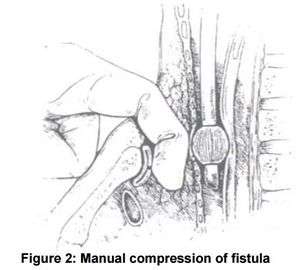
- Apply digital pressure of innominate artery against the manubrium from inside tracheostomy tract
- Go to the OR with finger tamponade innominate artery
- If above fails, place a cuffed ET tube to prevent pulmonary aspiration of blood
- Correct coagulopathies and administer blood products as needed
- Requires emergent OR exploration and definitive management
- Tracheoinnominate artery fistula (TIF) until proven otherwise
Disposition
- Emergent OR for TIF
- Most minor bleeds do not require admission and observation if controlled in ED
- Consult with primary surgeon for new tracheostomies
See Also
External Links
References
- https://www.ccam.net.au/handbook/tracheostomy/ Date accessed: 4/24/2018
- Allan JS, Wright CD. Tracheo-innominate fistula: diagnosis and management. Chest Surg Clin NA. 2003;13(2):331-41.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.