Tibial plateau fracture
Background
- ACL and MCL injuries associated with lateral plateau fracture
- PCL and LCL associated with medial plateau fracture
- Compartment syndrome may occur
- Segond fracture
- Avulsion fracture of margin of lateral tibial plateau just below joint line
- Associated with tear of ACL and meniscal ligaments
Clinical Features
- Occurs via axial load that drives femoral condyle into tibia
Differential Diagnosis
Acute knee injury
- Knee dislocation
- Knee fractures
- Meniscus and ligament knee injuries
- Patella dislocation
- Patellar tendonitis
- Patellar tendon rupture
- Quadriceps tendon rupture
Nontraumatic/Subacute
- Arthritis
- Gout and Pseudogout
- Osgood-Schlatter disease
- Patellofemoral syndrome (Runner's Knee)
- Patellar tendonitis (Jumper's knee)
- Pes anserine bursitis
- Popliteal cyst (Bakers cyst)
- Prepatellar bursitis (nonseptic)
- Septic bursitis
- Septic joint
- DVT
Evaluation
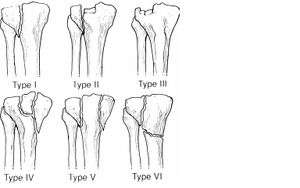
Schatzker Classification of Tibial Plateau Fractures
Imaging
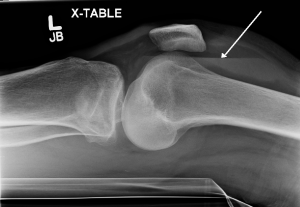
Lipohemarthrosis (presence of fat and blood from bone marrow in the joint space after an intraarticular fracture) seen on X-ray in a person with a subtle tibial plateau fracture
- AP, lateral, oblique views (internal for lateral plateau, external for medial plateau). Tunnel view may also be helpful.
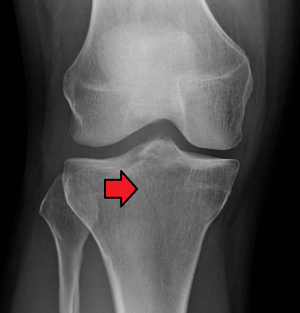
- AP - line drawn at lateral margin of femur should not have >5mm of tibia beyond it
- CT or MRI should be considered if plain film negative but high clinical suspicion based on mechanism or inability to bear weight
Schatzker Classification
- Schatzker I Lateral split
- Schatzker II Split with depression
- Schatzker III Pure lateral depression
- Schatzker IV Pure medial depression
- Schatzker V Bicondylar
- Schatzker VI Split extends to metadiaphysis
Management
General Fracture Management
- Acute pain management
- Open fractures require immediate IV antibiotics and urgent surgical washout
- Neurovascular compromise from fracture requires emergent reduction and/or orthopedic intervention
- Consider risk for compartment syndrome
Specific Management
- Knee immobilizer with non-weightbearing and ortho referral in 2-7d
- Emergent surgical management if open or if neurovascular compromise
Disposition
- Outpatient follow up
Indications for Expedited Referral (within 48hr)
- Significant displacement or depression
- Suspected or documented ligamentous injury
Indications for (outpatient) surgery
- Articular stepoff > 3mm
- Condylar widening > 5mm
- Varus/valgus instability
- All medial plateau fractures
- All bicondylar fractures
See Also
References
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.