Spinal cord injury
Background
- Penetrating injury
- GSW
- Most are stable injuries and only require supportive orthosis, analgesia
- Bullet removal does not improve neuro status for stable cervical and thoracic lesions
- Bullet removal may improve neuro status for thoracolumbar region injury (T11-L2)
- Stabbing
- Vertebral instability is generally not an issue
- Delayed deficits are rare
- If do occur related to retained fragment of blade within spinal canal
- GSW
Anatomy
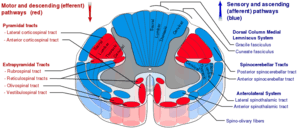
Spinal cord tracts
- Dorsal columns
- Proprioception, vibration
- Decussation at medulla
- Corticospinal Tract
- Voluntary motor
- Upper extremity fibers more central, lower extremity fibers more lateral
- Decussation at medulla
- Voluntary motor
- Spinothalamic
- Crude touch, pressure, pain, temperature
- Decussates 1-2 levels above entry point to spinal cord
Peds
- In patients <10yr spinal injury occurs mainly in upper cervical vertebrae
- In patients >10yr majority of injuries occur in lower cervical spine, similar to adults
- Odontoid fractures are among most common cervical spine injuries in children
- Do not confuse with normal anatomic variations in odontoid seen in children up to 7yr old
- SCIWORA
- Spinal cord injury without radiologic abnormality
- MRI has shown significant pathology in many of these patients
- Symptoms
- Delayed onset (within 48hr) of numbness, paresthesias in extremities
- Transient quadriparesis ("stinger")
- Occurs most often in boys after sports injuries
- Paresthesias or weakness of extremities lasting from seconds to minutes
- Complete recovery within 48hr
Types
Spinal Cord Syndromes
Differential Diagnosis
Evaluation
- Clinical (see spinal cord syndromes)
- X-ray
- See C-spine (NEXUS) and C-Spine X-Ray
- Consider:
- CT
- MRI
Management
- Consider intubation injuries at C5 or above
- Consider surgical intervention for:
- Progressive neurologic deficits
- Unstable spine fractures
- Steroids are no longer recommended
Administration of methylprednisolone (MP) for the treatment of acute spinal cord injury (SCI) is not recommended. Clinicians considering MP therapy should bear in mind that the drug is not Food and Drug Administration (FDA) approved for this application. There is no Class I or Class II medical evidence supporting the clinical benefit of MP in the treatment of acute SCI. Scattered reports of Class III evidence claim inconsistent effects likely related to random chance or selection bias. However, Class I, II, and III evidence exists that high-dose steroids are associated with harmful side effects including death.
[1]- See EBQ:High Dose Steroids in Cord Injury for further discussion
Disposition
- Admit
See Also
- Spinal Cord Levels
- Spinal cord compression (non-traumatic)
- Focal neurologic deficits
- Neurogenic Shock
- Spinal Shock
- Autonomic dysreflexia
- Thoracic and Lumbar Spine Injuries
References
- Hurlbert RJ et al. Pharmacological therapy for acute spinal cord injury. Neurosurgery. 2013 Mar;72 Suppl 2:93-105 http://www.ncbi.nlm.nih.gov/pubmed/23417182
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.