Skull fracture
This page is for adult patients; for pediatric patients see skull fracture (peds)
Background
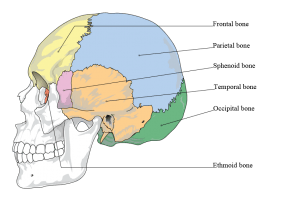
Bones of the cranium.
- Presence of skull fracture significantly increases risk of underlying intracranial injury
Clinical Features
Linear Skull Fracture
- Often have scalp hematoma or tenderness to palpation
Depressed Skull Fracture
- Depression or crepitus may be palpable on physical exam
Basilar Skull Fracture
- Raccoon eyes
- Battle sign
- Hemotympanum
- Clear rhinorrhea or otorrhea may indicate CSF leak from dural tear associated with fracture
Differential Diagnosis
Head trauma
- Traumatic brain injury
- Orbital trauma
- Maxillofacial trauma
- Skull fracture
- Pediatric head trauma
Evaluation
- CT head
- CBC
- Coags
- Evaluate for additional injuries
Management
Linear Skull Fracture
- If no intracranial bleed or other injuries, observe for 4-6 hrs and discharge
- Patients with advanced age, coagulopathy, or other co-morbidities may benefit from admission
Depressed Skull Fracture
- Neurosurgery consult
- Antibiotics, seizure prophylaxis (e.g. Keppra), surgery/wound debridement may be indicated in discussion with a neurosurgeon
Basilar Skull Fracture
- Neurosurgery consult
- Antibiotic prophylaxis is often started in setting of CSF leak but should be discussed with a neurosurgeon
Disposition
- Admit - except for simple linear skull fracture with no other injuries
See Also
External Links
References
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.