Rhabdomyolysis
Background
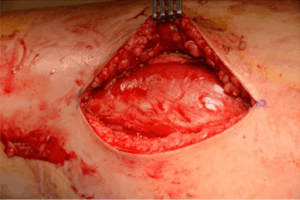
Intraoperative photograph of the left anterior compartment of the thigh. The quadriceps musculature can be seen bulging through the fascial defects.
- Muscle necrosis and release of intracellular muscle constituents into the circulation
- Recurrent episodes suggests inherited metabolic disorder
- Alcohol and drugs play a role in up to 80% of cases
Etiology
- Trauma or muscle compression
- Crush Syndrome
- Immobilization
- Compartment Syndrome
- Nontraumatic Exertional
- Exercise + hot weather
- Exercise + sickle cell
- Exercise + Hypokalemia
- Hyperkinetic states
- Seizure
- DTs
- Stimulant / Sympathomimetic[1] overdose
- Malignant Hyperthermia
- Neuroleptic malignant syndrome
- Nontraumatic Nonexertional
- Drugs and toxins
- Coma induced by sedatives
- Alcohol
- Statins
- Colchicine
- CO Poisoning
- Infection
- Endocrine
- Inflammatory myopathies
- Moderate CK elevations only (rhabdomyolysis only described in case reports)
- Miscellaneous
- Status Asthmaticus
- Toxic shock syndrome
- Mushroom ingestion
- Drugs and toxins
Clinical Features

Urine from a person with rhabdomyolysis showing the characteristic brown discoloration as a result of myoglobinuria
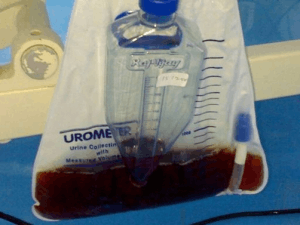
Tea coloured with severe rhabdomyolysis
- Myalgia, stiffness, weakness, malaise, low-grade fever, dark urine
- Musculoskeletal symptoms may be present in only half of cases
- Nausea and vomiting, abdominal pain, tachycardia in severe cases
- Mental status changes secondary to urea-induced encephalopathy
Differential Diagnosis
Red Urine
- Hematuria
- Hemoglobinuria
- Porphyria
- Myoglobinuria (rhabdomyolysis)
- Foods
- Blackberries
- Beets
- Blackberries
- Rhubarb
- Food coloring
- Fava beans
- Drugs
Evaluation
Work-up
- Obtain immediate ECG (electrolyte abnormalities)
- Total CK
- Urinalysis
- CBC
- Chemistry, including Mag, Phos
- Uric acid
- LFTs
- DIC panel
- Coags, FSP, fibrinogen
Evaluation
- Total CK
- Most consider rhabdomyolysis if 5x or greater increase above upper limit of normal (~2000)
- Serum CK begins to rise 2-12hr after injury, peaks within 24-72hr
- Degree of CK elevation correlates with muscle injury, but NOT renal failure
- CK-MB
- May be normal or mildly elevated (<5% of total)
- Uric Acid - elevates before CK
- Myoglobinuria
- Urinalysis = +blood, no RBCs (Sn ~80%)
- Myoglobin is cleared within 1-6hr (often see elevated CK with no myoglobinuria)
- Acute renal failure
- Creatinine increase
- Electrolyte abnormalities
- Hyperkalemia
- Hyperphosphatemia
- Hypocalcemia
- Hyperuricemia
Management
Trend:
- Volume status
- Urine pH
- Chemistry
- CK
- Calcium, phosphorus
IV Fluids
- Start with NS 1-2 L/hr
- After rapid correction of fluid deficit, one method is infusing 2.5 mL/kg/hr with urine output goal of 200-300 ml/hr (2-3 cc/kg/hr)
- Frequently need ~10 L/day
Urinary alkalinization
- Administered as bicarbonate drip
- Mix 150 mL [3 amps] of 8.4% sodium bicarbonate with 1 L D5W
- Infuse at 200 mL/hour; rate is adjusted to achieve urine pH of >6.5
- Controversial; no RCT to date have demonstrated benefit
- Consider if CK >5000, severe muscle injury (crush injury), rising CK AND urine pH <6.5
- Contraindications:
- Severe hypocalcemia
- Arterial pH > 7.50
- Serum bicarbonate > 30 meq/L
- Arterial pH and serum calcium should be monitored q2hr
- Discontinue alkalinization:
- Urine pH does not rise above 6.5 after 3-4hr
- Patient develops symptomatic hypocalcemia
- Arterial pH > 7.5
- Serum bicarbonate >30 meq/L
Mannitol
- Mannitol administration can worsen dehydration and oliguria and although used in the past should generally be avoided
- No RCT to date has demonstrated benefit
Intubation/RSI
- Use Rocuronium due to the potential elevations in potassium that result from the rhabdomyolysis
Disposition
- Discharge if:
- Exertional rhabdo
- Otherwise healthy
- No comorbidities (heat stress, dehydration, trauma)
- Downtrending total CK
- Consider admission for CK >30,000
- Otherwise admit to monitored bed
Complications
- Acute Renal Failure
- Neither presence of myoglobinuria nor degree of CK rise is predictive of ARF
- Rare in exertional rhabdomyolysis with out presence of dehydration, heat stress, trauma
- Most commonly oliguric
- Hyperkalemia
- Renal function, not release of K+, is most important determinant
- Treat aggressively; insulin may be ineffective; may require dialysis
- Hypocalcemia (initial phase)
- Treat only if symptomatic or severely hyperkalemic (often have rebound hypercalcemia)
- Hypercalcemia (recovery phase)
- Hyperphosphatemia
- Treat cautiously (treatment may worsen calcium precipitation in muscle)
- Consider oral phosphate binders when level >7
- DIC
- Usually resolves spontaneously within several days
- Compartment Syndrome
- Peripheral nerve injury
- Usually resolves within few days-weeks
See Also
References
- O'Connor AD et al. Prevalence of Rhabdomyolysis in Sympathomimetic Toxicity: A Comparison of Stimulants. J Med. Toxicol. 2015;11(2)195-200
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.