Retropharyngeal abscess
Background
- Polymicrobial abscess in space between posterior pharyngeal wall and prevertebral fascia
- Adults: Due to direct extension of purulent debris from adjacent site (e.g. Ludwig's angina)
- More likely to extend into the mediastinum
- Children: Due to suppurative changes within a lymph node (primary infection elsewhere in head or neck)
- Trauma: Direct inoculation (e.g. child falling with stick in mouth)
- Patients may prefer to lay supine to prevent abscess and edematous posterior wall to collapse into airway, so patients should not be forced to sit up
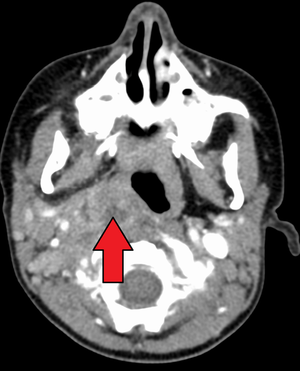
Retropharyngeal abscess on CT
Clinical Features
Initial symptoms
- Sore throat (76%)
- Fever (65%)
- Torticollis (37%)
- Dysphagia (35%)
Late symptoms
- Stridor, respiratory distress, chest pain (mediastinitis)
- Drooling, neck stiffness
- Involvement of carotid neurovascular sheath
Complications
- Mediastinitis, sepsis, aspiration from spontaneous abscess formation
- Jugular venous thrombosis, Lemierre's syndrome
Differential Diagnosis
Bacterial infections
- Streptococcal pharyngitis (Strep Throat)
- Neisseria gonorrhoeae
- Diphtheria (C. diptheriae)
- Bacterial Tracheitis
Viral infections
- Infectious mononucleosis (EBV)
- Patients with peritonsillar abscess have a 20% incidence of mononucleosis [1]
- Laryngitis
- Acute Bronchitis
- Rhinovirus
- Coronavirus
- Adenovirus
- Herpesvirus
- Influenza virus
- Coxsackie virus
- HIV (Acute Retroviral Syndrome)
Other
- Deep neck space infection
- Peritonsillar Abscess (PTA)
- Epiglottitis
- Kawasaki disease
- Penetrating injury
- Caustic ingestion
- Lemierre's syndrome
- Peritonsillar cellulitis
- Lymphoma
- Internal carotid artery aneurysm
- Oral Thrush
- Parotitis
- Post-tonsillectomy hemorrhage
- Vincent's angina
- Acute necrotizing ulcerative gingivitis
Pediatric stridor
- A minimal amount of edema or inflammation in the pediatric airway can result in significant obstruction
- Can lead to rapid decompensation
<6mo
- Laryngotracheomalacia
- Accounts for 60%
- Usually exacerbated by viral URI
- Dx w/ flexible fiberoptic laryngoscopy
- Vocal cord paralysis
- Stridor associated w/ feeding problems, hoarse voice, weak and/or changing cry
- May have cyanosis or apnea if bilateral (less common)
- Subglottic stenosis
- Congenital vs 2/2 prolonged intubation in premies
- Airway hemangioma
- Usually regresses by age 5
- Associated w/ skin hemangiomas in beard distribution
- Vascular ring/sling
>6mo
- Croup
- viral laryngotracheobronchitis
- 6 mo- 3 yr, peaks at 2 yrs
- Most severe on 3rd-4th day of illness
- Steeple sign not reliable- diagnose clinically
- Epiglottitis
- H flu type B
- Have higher suspicion in unvaccinated children
- Rapid onset sore throat, fever, drooling
- Difficult airway- call anesthesia/ ENT early
- H flu type B
- Bacterial tracheitis
- Rare but causes life-threatening obstruction
- Sx of croup + toxic-appearing = bacterial tracheitis
- Foreign body (sudden onset)
- Marked variation in quality or pattern of stridor
- Retropharyngeal abscess
- Fever, neck pain, dysphagia, muffled voice, drooling, neck stiffness/torticollis/extension
Evaluation

A lateral x-ray demonstrating prevertebral soft tissue swelling (marked by the arrow)
- CT neck with IV contrast
- Gold standard
- XR Soft tissue
- Neck in extension at end inspiration
- The prevertebral space should be less than 7mm at C2, 14mm at C6 in children regardless of the age
- The prevertebral space should be less than 22mm at C6 in adults
- The prevertebral space should be less than one-half the width of the corresponding vertebral body
- If equivocal XR, order CT
Management
- Emergent ENT consult
- Most patients require I&D
- Indications for drainage - trismus, rim enhancement on CT
- Secure airway - care must be taken to minimize contact with abscess as rupture is significant risk
- Tracheostomy or fiberoptic intubation may be necessary
- CT or MRI may help prepare for method of definitive airway[2]
Antibiotics
- Clindamycin 600-900mg IV OR
- Cefoxitin 2gm IV OR
- Ampicillin/Sulbactam 3g IV
Disposition
- Admit
See Also
- PTA
- Ludwig's Angina
- Pharyngitis
References
- Melio, Frantz, and Laurel Berge. “Upper Respiratory Tract Infection.” In Rosen’s Emergency Medicine., 8th ed. Vol. 1, n.d.
- Mulimani SM. Anesthetic management of tuberculous retropharyngeal abscess in adult. J Anaesthesiol Clin Pharmacol. 2012 Jan-Mar; 28(1): 128–129.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.