Radial head fracture (peds)
This page is for pediatric patients; see radial head fracture for adult patients.
Background
- Radial neck fractures tend to be more common in the pediatric population than radial head fractures
- Majority are Salter II fractures
- Average age is approximately 10 yrs
Clinical Features
- Mechanism is typically FOOSH
- Tenderness over the elbow
- May include posterior interosseous nerve intrapment causing a finger drop
Differential Diagnosis
Radiograph-Positive
- Distal humerus fracture
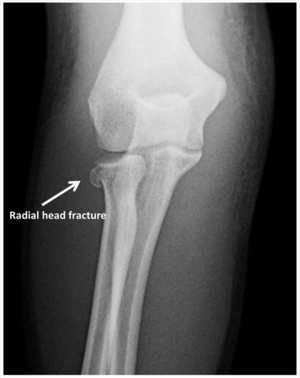
- Radial head fracture
- Capitellum fracture
- Olecranon fracture
- Elbow dislocation
Radiograph-Negative
- Lateral epicondylitis
- Medial epicondylitis
- Olecranon bursitis (nonseptic)
- Septic bursitis
- Biceps tendon rupture/dislocation
Evaluation
Workup
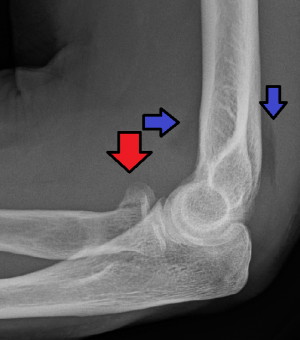
Radial head fracture (red arrow) with posterior and anterior sail sign (blue arrows).
- AP and lateral elbow xray
- Assess for anterior fat pad
Diagnosis
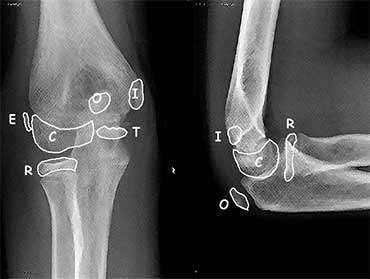
Knowledge of ossification centers of the elbow can be helpful (see Elbow X-ray)
Elbow Ossification by Age (CRITOE)
| Ossification Center | Age of Appearance (add 1yr for boys) |
| Capitellum | 1yr |
| Radial head | 3yr |
| Internal epicondyle | 5yr |
| Trochlea | 7yr |
| Olecranon | 9yr |
| External epicondyle | 11yr |
Management
General Fracture Management
- Acute pain management
- Open fractures require immediate IV antibiotics and urgent surgical washout
- Neurovascular compromise from fracture requires emergent reduction and/or orthopedic intervention
- Consider risk for compartment syndrome
Specific Management
- Ortho consultation to guide treatment
- ORIF indicated when angulation >60 degrees or displacement >50%
Disposition
- Consult ortho
See Also
External Links
References
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.