Perilunate and lunate dislocations
Background
- Occur via high-energy FOOSH injury (fall from height, MVC)
- Perilunate Dislocation = Lunate stays in place, capitate is displaced
- Lunate Dislocation = Capitate stays in place, lunate is displaced
- Commonly missed (~25%) on initial presentation
- Must rule-out median nerve injury
- Must rule out carpal bone fractures
Clinical Features
- Perilunate dislocation: dorsal swelling with palpable mass
- Lunate dislocation: volar swelling with palpable mass
Evaluation
Perilunate Dislocation
Lunate Dislocation
| Mayfield Classification | Level of carpal instability |
|---|---|
| Stage I: scapholunate dissociation | Disruption of scapholunate ligament with +Terry Thomas sign; exacerbated in clenched fist view |
| Stage II: perilunate dislocation | +Disruption of capitolunate joint; high association with scaphoid fractures |
| Stage III: midcarpal dislocation | +Disruption of triquetrolunate joint; neither capitate or lunate is aligned with distal radius |
| Stage IV: lunate dislocation | +Disruption of radiolunate joint |
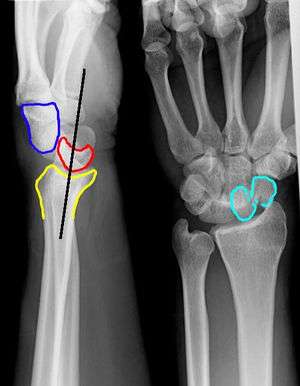
Perilunate Dislocation
- Lateral view
- Capitate displaced dorsal to lunate
- Lunate retains its normal contact with radius
- PA view
- Capitolunate joint space is obliterated as the bones overlap one another
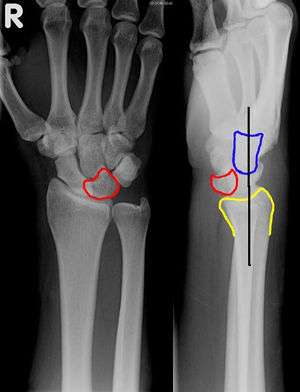
Lunate Dislocation
- Lateral view
- Lunate is pushed off the radius into the palm ("spilled teacup" sign)
- PA view
- Lunate has triangular shape ("piece-of-pie sign")
Differential Diagnosis

Management
- Closed reduction and long-arm splint
- Requires emergent ortho consultation (very difficult to reduce with high incidence of median nerve compression), and usually emergent operative management
See Also
References
- Emergency Orthopedics, The Extremeties
- Radiopaedia.org
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.