Paget's disease of bone
Background
- Characterized by areas of bone with excessive osteolytic activity and subsequent increased ostoblastic activity, resulting in disorganized bone formation
- Results in osteolytic lesions and weakened bone
- Eventually, affected bones may be abnormally enlarged
- Exact etiology unknown, likely genetic component
- Prevalence increases with age, more common in people of European descent
Clinical Features
Differential Diagnosis
- Bone tumor (e.g. osteosarcoma or metastesis)
- Multiple myeloma, myelofibrosis
- Fibrous dysplasia
- Intramedullary osteosclerosis
- Sickle cell disease
Malignant
- Multiple myeloma
- Chondrosarcoma
- Paget disease
- Osteosarcoma
- Adamantinoma
- Chordoma
- Primary bone lymphoma
- Fibrosarcoma
- Myosarcoma
Benign
- Giant cell tumor
- Chrondroblastoma
- Enchondroma
- Langerhans cell histiocytosis of bone
- Osteoblastoma
- Osteochondroma
- Osteoid osteoma
Evaluation

Paget's disease of right innominate bone.
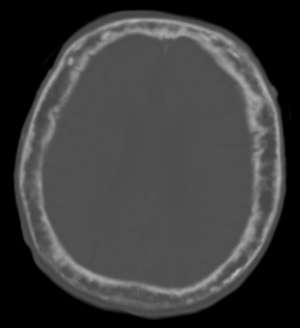
Skull CT showing “cotton wool spots” typical of later stages of Paget’s disease.
- Imaging to evaluate for fractures
- Initial lesion may be destructive, radiolucent (especially in skull)
- Involved bones may be expanded, abnormally dense
- May have multiple fissure fractures in long bones
- Alk phos typically very high
- Serum calcium may be high
Management
- Treat fractures
- Pain control
- Bisphosphonates (e.g. Zoledronate) are treatment of choice for patients with severe symptoms or advanced disease
Disposition
- Discharge uncomplicated patients
See Also
External Links
References
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.