Transcutaneous pacing
Background
Indications
- Bradyarrythmias causing hemodynamic impairment:[1]
- AV block
- Sinus node dysfunction
- A-fib with slow ventricular response
- Malfunction of implanted pacemaker
- Tachyarrhythmias causing hemodynamic impairment[1]
Procedure
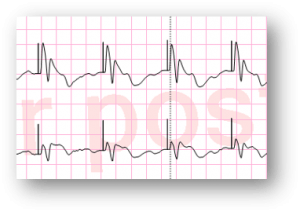
True electrical capture
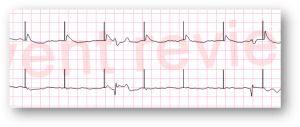
False capture with visible phantom beats[2]
- Pad placement:
- Pad on apex of heart and on right upper chest
- Pad on lead V3 position and between left scapula and T-spine
- Set: HR 80, pacing threshold usually between 40-80 mA
- If hemodynamically unstable or with evidence of end organ poor perfusion start at 80 mA and titrate down as tolerated.
- Look for clear QRS complex and T-wave following pacer spike
- Check pulse to confirm mechanical capture
- Final current set 5-10 mA above threshold level for patient
See Also
References
- Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation. May 27 2008;117(21):e350-408
- "Transcutaneous Pacing (TCP): The Problem of False Capture". EMS 12 Lead. Retrieved 2019-01-31.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.