Acute otitis media
Background
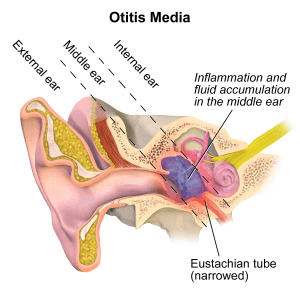
Anatomy of acute otitis media.
- Peak incidence: 6-18 months of age
- 2nd most common cause of ED visits after URI
Clinical Features

A bulging tympanic membrane which is typical in a case of acute otitis media
Differential Diagnosis
External
- Auricular hematoma
- Auricular perichondritis
- Cholesteatoma
- Contact dermatitis
- Ear foreign body
- Herpes zoster oticus (Ramsay Hunt syndrome)
- Malignant otitis externa
- Otitis externa
- Otomycosis
- Tympanic membrane rupture
Inner/vestibular
Less common
- Oral cavity disease (referred pain)
- Cholesteatoma
- PTA
- Brain abscess
- Lemierre's Syndrome
- Herpes zoster oticus
Pediatric fever
Evaluation
- Typically clinical
- Erythema alone not enough to diagnose
- Other clinical features: acute onset pain, bulging TM, opacified TM/loss of landmarks, otorrhea
Management
Analgesia
- Acetaminophen/ibuprofen and topical benzocaine (unless perforated TM)
2013 AAP Decision to Treat Guidelines[1]
| Age | Otorrhea | Severe Symptoms^ | Bilateral without Otorrhea | Unilateral without Otorrhea |
| 6mo-2y | Antibiotics | Antibiotics | Antibiotics | Antibiotics or observation period (wait and see) |
| ≥2y | Antibiotics | Antibiotics | Antibiotics or observation period (wait and see) | Antibiotics or observation period (wait and see) |
^Fever > 39C or severe otalgia <48 hrs
Also Consider In:
- Age <6mo
- Ill-appearing
- Recurrent acute otitis media (within 2-4wk)
- Concurrent antibiotic treatment
- Other bacterial infections
- Immunocompromised
- Craniofacial abnormalities
Wait-and-see antibiotic prescription (WASP)
- Rather that routine prescription is an option to avoid over use if the patient does not meet any of the prescription criteria[2]
- If symptoms worsen or persist for 48-72 then caretaker fill the prescription
- Fever (relative risk [RR], 2.95; 95% confidence interval [CI], 1.75 - 4.99; P<.001) and otalgia (RR, 1.62; 95% CI, 1.26 - 2.03; P<.001) were associated with filling the prescription in the WASP group
Antibiotics Options
- Consider treating for a standard of 10 days as opposed to a shorter duration of 5 days to reduce treatment failure in young children[3]
- Treatment failure for 10 day at 16% and for 5 day at 34% for amoxicillin-clavulanate
- RTC of 520 children aged 6-23 months
Treatment during prior Month
- If amoxicillin taken in past 30 days, Amoxicillin/Clavulanate
- 80-90mg of amoxicillin per kg/day PO divided BID x 7-10 days
- Clavulanate increases vomiting/diarrhea
- Cefdinir 14mg/kg/day BID x7-10 days
- Cefpodoxime 10mg/kg PO daily x7-10 days
- Cefuroxime 15mg/kg PO BID x7-10 days
- Cefprozil 15mg/kg PO BID x7-10 days
Otitis/Conjunctivitis
- Suggestive of non-typeable H.flu
- Amoxicillin/Clavulanate
- 80-90mg of amoxicillin per kg/day PO divided BID x 7-10 days
- Clavulanate increases vomiting/diarrhea
Treatment Failure
defined as treatment during the prior 7-10 days
- Amoxicillin/Clavulanate
- 80-90mg of amoxicillin per kg/day PO divided BID x 7-10 days
- Ceftriaxone 50mg/kg IM once as single injection x 3 days
- Use if cannot tolerate PO
Penicillin Allergy
- Azithromycin 10mg/kg/day x 1 day and 5mg/kg/day x 4 remaining days
- Clarithromycin 7.5mg/kg PO BID x 10 days
- Clindamycin 10mg/kg PO three times daily
- Clindamycin does not cover H. influenza and M. catarrhalis and treatment should favor Azithromycin use
Disposition
- Outpatient management
Complications
- Mastoiditis
- Meningitis
- Brain Abscess
- Lateral Sinus Thrombosis
See Also
References
- AAP Clinical Practice Guideline The Diagnosis and Management of Acute Otitis Media http://pediatrics.aappublications.org/content/early/2013/02/20/peds.2012-3488.full.pdf
- Spiro DM. Wait-and-see prescription for the treatment of acute otitis media: a randomized controlled trial. JAMA. 2006 Sep 13;296(10):1235-41.
- Hoberman A et al. Shortened Antimicrobial Treatment for Acute Otitis Media in Young Children. N Engl J Med 2016; 375:2446-2456.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.