Osgood-Schlatter disease
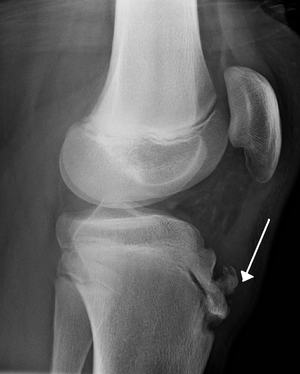
Lateral view X-ray of the knee tibial with overlying soft tissue swelling.
Background
- Apophysitis of tibial tubercle resulting from repeated normal stresses or overuse
- Patients are usually 10-15yr old
- More commonly occurs in running or jumping athletes
Clinical Features
- Most cases are bilateral
- Although symptoms are commonly asymmetric
- Chronic, intermittent pain over the anterior aspect of knee and tibial tuberosity
- Pain aggravated by activity, improves with rest
- Prominence and soft tissue swelling over tibial tubercle
Differential Diagnosis
Acute knee injury
- Knee dislocation
- Knee fractures
- Meniscus and ligament knee injuries
- Patella dislocation
- Patellar tendonitis
- Patellar tendon rupture
- Quadriceps tendon rupture
Nontraumatic/Subacute
- Arthritis
- Gout and Pseudogout
- Osgood-Schlatter disease
- Patellofemoral syndrome (Runner's Knee)
- Patellar tendonitis (Jumper's knee)
- Pes anserine bursitis
- Popliteal cyst (Bakers cyst)
- Prepatellar bursitis (nonseptic)
- Septic bursitis
- Septic joint
- DVT
Evaluation
- Imaging is not typically necessary
- If obtained shows nonspecific irregularities of tibial tubercle
- Indications for knee xrays (to evaluate for avulsion fracture of the tibial epiphysis)
- Swelling
- Inability to actively extent the knee
- decreased strength with knee extension, or inability to walk
Management
- Disease is self-limited
- Most patients' symptoms respond to rest and temporary avoidance of offending activity
- Complete avoidance of activity is not essential
- Immobilization is contraindicated
- NSAIDs
- Apply ice after activity
Disposition
Discharge
See Also
References
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.