Mid-shaft femur fracture
Includes all subtrochanteric femur fractures
Background
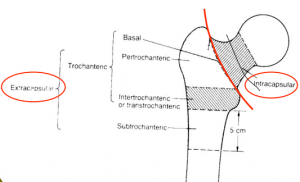
Location of femur fractures
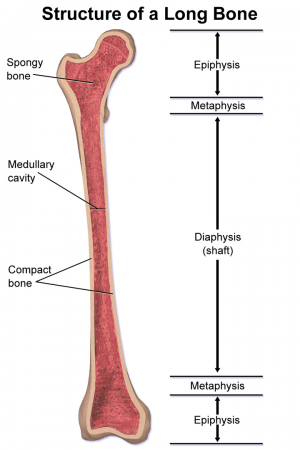 Long bone anatomy.
Long bone anatomy.- Occurs with severe trauma or in association with pathologic bone
- Blood loss can be substantial (average loss = 1L)
Clinical Features
- Clinical presentation is similar to intertrochanteric fracture
- Affected leg is shortened and externally rotated
Differential Diagnosis
Proximal
- Intracapsular
- Extracapsular
Evaluation

Spiral shaft fracture of femur.
Workup
- Radiography
- Obtain films of knee, femur, and hip for operative planning and to assess for other injury
- Pre-op labs
- CBC
- Chem 7
- PT/PTT
- Type & Screen
Diagnosis
- Typically via plain films
Management
- Resuscitation per ATLS guidelines
General Fracture Management
- Acute pain management
- Open fractures require immediate IV antibiotics and urgent surgical washout
- Neurovascular compromise from fracture requires emergent reduction and/or orthopedic intervention
- Consider risk for compartment syndrome
Immobilization
- Consider traction splint
- Little evidence to support its use[1]
- Theoretical benefit of traction splinting is reduction in bleeding and improved pain
- Sager and Hare splints are commonly used by EMS providers
- Buck's traction used by ortho
Disposition
- Admit
- Typically requires ORIF
See Also
External Links
References
- Agrawal Y, Karwa J, Shah N, et al. Traction splint: to use or not to use. J Perioper Pract. 2009; 19(9):295-298.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.