Measles
Background
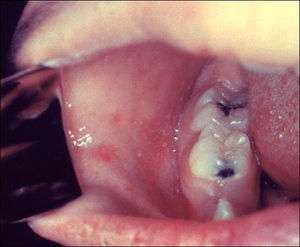
Koplik's Spots on Cheek

Koplik's Spots on Palate

Measle's Rash on Face

Measle's Rash on on Thorax
- Also known as Rubeola, which is not to be confused with German Measles (Rubella)
- Patients are contagious from about 4 days before to 4 days after onset of rash
Clinical Features
- Consider measles in a patient of any age who has an acute RASH and FEVER
- Risk factors
- In the prior 3 weeks: travel outside of North America, transit through U.S. international airports, interaction with foreign visitors, including at a U.S. tourist attraction, or travel to areas of the U.S with ongoing measles transmission.
- Confirmed measles cases in your community.
- Never immunized with measles vaccine and born in 1957 or later.
- Incubation period - 10 days
- Prodrome of high fever, cough, coryza, and conjunctivitis (lasts ~3 days)
- Koplik's spots (appears day 2-3) - pathognomonic enanthem
- Tiny red spots (base) with bluish-white centers on the mucosa of the cheek or palate
- Rash (begins day 4 - lasts to day 7)
- Red, blotchy, and maculopapular; rapidly progresses to confluence
- Usually starts on the face (hairline and behind the ears)
- Rapidly spreads to the chest, back, and finally the legs and feet
- Rash resolves in order of appearance between days 7-9
Complications
- Secondary infection
- Measles virus can directly infect T cells, leading to systemic immune suppression and secondary infections
- Gastrointestinal
- Diarrhea is the most common complication
- Others: gingivostomatitis, gastroenteritis, hepatitis, mesenteric lymphadenitis, and appendicitis
- Pulmonary
- Pneumonia is the most common cause of measles-associated death in children
- Neurologic
- Encephalitis
- Acute disseminated encephalomyelitis
- Demyelinating disease thought to be a postinfectious autoimmune response
- Subacute sclerosing panencephalitis
- A fatal, progressive degenerative disease of the CNS that usually occurs 7 to 10 years after natural measles virus infection
Differential Diagnosis
Evaluation
Workup
Initial treatment/isolation is based on clinical suspicion; testing is normally performed in conjunction with recommendations by local public health experts[1]
Diagnosis[1]
Providers should consider measles in patients with FEVER AND a descending RASH in a person with a history of travel or contact with someone who has travelled outside North America whether or not the patient has had 2 doses of MMR or prior measles disease. However, persons without a history of travel or exposure to a traveler, are unlikely to have measles in the absence of confirmed measles cases in your community.
Management
- Supportive care
Suspected Active Measles Case[1]
- Isolate patient immediately (see below)
- Alert your local health department immediately
- The risk of measles transmission to others and large contact investigations can be reduced if control measures are implemented immediately
- If advised to test for measles by your local health department, submit a specimen for polymerase chain reaction (PCR) testing (see Workup section above).
Isolation Precautions
- For suspected patients
- Mask the patient and isolate immediately in an airborne infection isolation room
- All personnel entering the room should use respiratory protection at least as effective as an N95 respirator
- If possible, allow only personnel with documentation of 2 doses of live measles vaccine or laboratory evidence of immunity (measles IgG positive) to enter the room
- Do not use the room for at least 2 hours after the patient leaves.
Post-Exposure Prophylaxis (Non-Immune Contact)
- Immunocompetent:
- MMR Vaccine (within 72 hours of exposure)
- Immunocompromised, children <12 months, and others at high risk of complications:
- IM Immune globulin (up to 6 days after exposure)
- Consider checking with your local health authorities
Disposition
- Discuss with public health
- Patients may be admitted with isolation to prevent public health spread vs. discharged with home isolation precautions
See Also
- Pediatric Rashes
External Links
- Guidance from CDC for healthcare professionals: https://www.cdc.gov/measles/hcp/index.html
- CDC clinical syndromes: https://www.cdc.gov/vaccines/pubs/pinkbook/meas.html
References
- California Department of Public Health Health Advisory: Measles Clinical Guidance: Identification and Testing of Suspect Measles Cases. April 3, 2019
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.