Liver injury
Background
- Occurs in 5% of all traumas
- Most common abdominal injury
Clinical Features
Differential Diagnosis
Evaluation
ATLS Blunt Abdominal Trauma Algorithm
- Unstable
- FAST to search for free fluid (vs. DPL if unavailable)
- Positive: Exploratory laparotomy
- Negative: CT scan
- FAST to search for free fluid (vs. DPL if unavailable)
- Stable
- CT scan
- Exploratory laparotomy, angiographic embolization, conservative management as indicated
- CT scan
American Association for the Surgery of Trauma Grading System
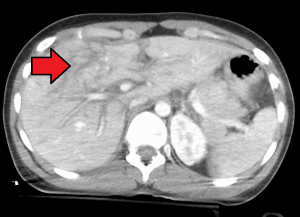
Grade 4 liver laceration (arrow).
| Grade^ | Hematoma | Laceration |
|---|---|---|
| I |
|
|
| II |
|
|
| III |
|
|
| IV |
|
|
| V |
|
|
| VI |
|
- ^Advance one grade for multiple injuries up to grade III
Management
- Nonoperative management is successful in >90% of patients who are hemodynamically stable
- Low-grade injuries (grades I–III) can almost always be managed without surgery
- Higher-grade injuries commonly fail nonoperative therapy.
- Consider angiographic embolization if:
- Large amount of hemoperitoneum
- Vascular injury (contrast blush) on CT
Disposition
- Typically admission via OR, IR, or floor/ICU for conservative management
See Also
References
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.