Canthotomy
Background
- Acute orbital compartment syndrome (OCS) is a clinical diagnosis
- Vision loss can be permanent after 60-100 min of ischemia[1] - do not delay procedure for imaging[2]
Causes[1]
- Trauma (retrobulbar hematoma) - most common cause
- Spontaneous bleed
- Tumor
- Orbital cellulitis/abscess
- Prolonged hypoxemia
Indications[3]
- Suspected acute orbital compartment syndrome (OCS), plus one or more of the following:
- Decreased visual acuity
- IOP >40 or marked difference in globe compressibility by palpation
- Proptosis
- Secondary indications (subjective and nonspecific) - if only secondary indications are present, get emergent ophthalmology consult prior to performing canthotomy.
- Afferent pupillary defect
- Cherry red macula
- Ophthalmoplegia
- Nerve head pallor
- Significant eye pain
Contraindications
- Globe Rupture
Equipment
- Betadine prep
- Sterile drape or towels
- Lidocaine with epi
- Syringe with 27-30ga needle
- Normal saline for irrigation
- Straight hemostat or needle driver
- Iris or suture scissors
- Forceps
Procedure[1][3][4]
Consider sedating patient for procedure, if time allows
- Prep and drape the area (Irrigation with normal saline is acceptable prep given emergent nature of procedure)
- Inject lidocaine with epinephrine into the lateral canthus directing the needle tip toward the lateral orbital rim (away from the globe)
- Apply hemostat to the lateral canthus from the angle of the eye to the orbital rim and clamp shut for ~1 min. (provides relative devascularization as well as a landmark for the canthotomy)
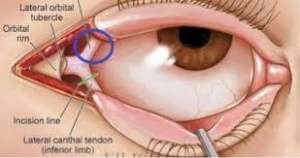
- Using scissors, incise the lateral canthus from the angle of the eyelid to the orbital rim (~1cm).
- Retract the inferior lid and bluntly dissect tissue until the canthal tendon is identified.
- Perform inferior cantholysis - cut the inferior crus of the lateral canthus tendon (point scissors infero-posteriorally toward the lateral orbital rim, avoiding the globe)
- Recheck IOP → if still elevated, perform superior cantholysis - cut the superior crus of the canthal tendon (some experts recommend performing both inferior and superior cantholysis at the same time, prior to re-evaluating IOP)
Complications
- Incomplete cantholysis
- Iatrogenic globe or surrounding structure injury (rare)
- Loss of adequate lower lid suspension
- Bleeding
- Infection
See Also
External Links
EMRAP procedure video- https://www.youtube.com/watch?v=tgQaKVGynFA
References
- Rowh AD, Ufberg JW, Chan TC, et al. Lateral canthotomy and cantholysis: emergency management of orbital compartment syndrome. J Emerg Med. 2015 Mar;48(3):325-30.
- Mohammadi F, Rashan A, Psaltis A, et al. Intraocular Pressure Changes in Emergent Surgical Decompression of Orbital Compartment Syndrome. JAMA Otolaryngol Head Neck Surg. 2015 Jun 1;141(6):562-5.
- McInnes G, Howes DW. Lateral canthotomy and cantholysis: a simple, vision-saving procedure. CJEM. 2002 Jan;4(1):49-52.
- Ballard SR, Enzenauer RW, O'Donnell T, et al. Emergency lateral canthotomy and cantholysis: a simple procedure to preserve vision from sight threatening orbital hemorrhage. J Spec Oper Med. 2009 Summer;9(3):26-32.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.