Lactic acidosis
Background
- Most common cause of metabolic acidosis in hospitalized patients
Clinical Features
- Anorexia
- Nausea
- Vomiting
- Abdominal pain
- Lethargy
- Hyperventilation
- Hypotension
Differential Diagnosis
By Type
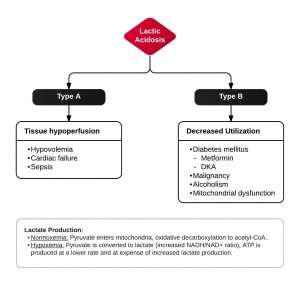
- Type A (tissue hypoperfusion)
- Hypovolemia
- Cardiac failure
- Sepsis
- Type B (decreased utilization)
- Alcoholism
- ↓ Lactate utilization secondary to hepatic dysfunction
- ↓ NAD+/NADH ratio leads to ↑ conversion of pyruvate to lactate
- Metformin
- DKA
- Mainly due to D-lactate production, though hypovolemia contributes
- Liver disease (decreased clearance)
- Adrenergic receptor agonism; viz., albuterol, epinephrine, etc
- Malignancy
- Carbon Monoxide poisoning
- Cyanide poisoning
- Alcoholism
- Type D
- episodes of encephalopathy and metabolic acidosis typically following high carbohydrate meals in patients with short bowel syndrome
- metabolic acidosis and high serum anion gap, normal lactate level, short bowel syn or other forms of malabsorption, and characteristic neurologic findings
- Type D lactate is not detected with standard lactate levels
Complete List
- Any shock state
- SIRS; lactate may be 2-5 mEq/L
- Thiamine deficiency; more often seen in ICU settings; Thiamine is a co-factor for pyruvate dehydrogenase
- Seizure
- Dead gut
- Hepatic failure
- Malignancy
- Exercise
- Albuterol and other beta agonists[1]
- Toxicologic Causes:
- Cyanide
- Carbon Monoxide
- Metformin
- Didanosine
- Stavudine
- Zidovudine
- Linezolid
- Strychnine
- Emtriva
- Rotenone (Fish Poison
- NaAzide (Lab Workers)
- APAP (if Liver Fx)
- Phospine (rodenticide)
- NaMonofluoroacetate (Coyote Poison‐ give Etoh as antidote)
- INH (if patient seizes)
- Hemlock
- Valproate
- Hydrogen Sulfide
- Nitroprusside (if cyanide toxic)
- Ricin & Castor Beans
- Propofol
- Sympathomimetics (cocaine, methamphetamine)
- Jequirty peas (Abrus precatorius)
- Prunus Amygdalus plants
- Crab tree apple seeds & cassava (yucca)
- HAART-induced lactic acidosis
Evaluation
- Hyperlactatemia = Lactate >2 mEq/L
- Lactic Acidosis = Lactate >4 mEq/L
Lactate False Positives
- Beta agonists or beta stimulation
- Extreme exercise
- Seizures, immediate ictal period
- Hepatic failure
- Lactate ringer's solution unlikely to cause false positive except in hepatic failure
Management
- Treat underlying cause
Disposition
- Depends on underlying cause
References
- Dodda V and Spiro P. Albuterol, an Uncommonly Recognized Culprit in Lactic Acidosis. Chest. 2011;140.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.