Laceration repair
Indications
- Skin or mucosal laceration.
Contraindications
- Body laceration >12 hours old
- Face/scalp wounds >24 hours old
Management
Wound Preparation
- Debridement is most important step in reducing infection/ promoting healing
- Avoid betadine/chlorhexadine in wound
- Not necessary to remove hair as this can increase chances of infection (if do, avoid using razor)
- Can use antibiotic ointment to help keep hair out of the way
Irrigation
- High pressure irrigation is best (can be achieved with 18 gauge syringe)
- Tap water is as effective as sterile water/ normal saline[1][2][3]
- Pressure from tap is ~45 psi, higher than syringe[4]
- Irrigation optional for face/scalp wound as long as:
- Not a bite wound
- Not a contaminated wound
- Not older than 6 hours
- Often best to avoid irrigation of face and opt for cleaning with gauze to help prevent tissue distortion
Anesthesia
- Can be topical or injected.
- Topical
- Evaluate motor/sensation before giving local anesthesia
- To decrease pain of injection:
- Buffer lidocaine with bicarbonate (1mL bicarb:9mL lidocaine)
- Inject slowly
- Consider nerve blocks to avoid tissue distortion for cosmetic areas such as vermillion border
- Also helpful for extremities, sole of foot
- Digital block for finger lacerations
Maximum Doses of Anesthetic Agents
| Agent | Without Epinephrine | With Epinephrine | Duration | Notes |
| Lidocaine | 5 mg/kg (max 300mg) | 7 mg/kg (max 500mg) | 30-90 min |
|
| Mepivicaine | 7 mg/kg | 8 mg/kg | ||
| Bupivicaine | 2.5 mg/kg (max 175mg) | 3 mg/kg (max 225mg) | 6-8 hr |
|
| Ropivacaine | 3 mg/kg | |||
| Prilocaine | 6 mg/kg | |||
| Tetracaine | 1 mg/kg | 1.5 mg/kg | 3hrs (10hrs with epi) | |
| Procaine | 7 mg/kg | 10 mg/kg | 30min (90min with epi) |
Exploration
- See Soft tissue foreign body
- Explore to base of wound
- Ideally done in bloodless field
- Look for foreign bodies, tendon injury, or fracture
- Possible glass or metal in wound = get XR or US to evaluate
Suturing
- See Sutures
- If laceration not closed immediately secondary to age of wound:
- Irrigate and explore wound, then pack with non-adherent or vaseline gauze
- Re-check in 3 days - may suture at that point if wound appears clean.
Sutures chart
| Area | Size | Type | Days to Removal |
|---|---|---|---|
| Scalp | Staples or 4-0 or 5-0 | non absorbable | 7 |
| Ear | 6-0 | non absorbable | 5-7 |
| Eyelid | 6-0 or 7-0 | absorbable or nonabsorbable | 5-7 |
| Eyebrow | 5-0 or 6-0 | absorbable or nonabsorbable | 5-7 |
| Nose | 6-0 | absorbable or nonabsorbable | 5-7 |
| Lip | 6-0 | absorbable | NA |
| Oral mucosa | 5-0 | absorbable | NA |
| Other face / forehead | 6-0 | absorbable or nonabsorbable | 5 |
| Chest/abdomen | 4-0 or 5-0 | non absorbable | 12-14 |
| Back | 4-0 or 5-0 | non absorbable | 7-10 |
| Extremities | 4-0 or 5-0 | non absobrable | 7-10 |
| Hand | 5-0 | non absorbable | 7-10 |
| Foot / Sole | 4-0 | non absorable | 12-14 |
| Joint (Extensor) | 4-0 | non absorable | 10-14 |
| Joint (Flexor) | 4-0 | non absorbable | 7-10 |
| Vagina | 4-0 | absorbable | NA |
| Penis | 5-0 | non absorbable | 7-10 |
| Scrotum | 5-0 | non absorbable | 7-10 |
Note: consider use of Fast Absorbing Gut (5-0/6-0) on Ear, Eyelid, Eyebrow, Nose, Lip and Face if anticipated difficulty with suture removal
Note: Favor absorbable sutures for facial repair especially in children
Steri-Strips
- Just as good a suturing according to this [6] and other articles. Picture on how to do it property from the same article [6] which is under CC BY-NC-SA 4.0 license:
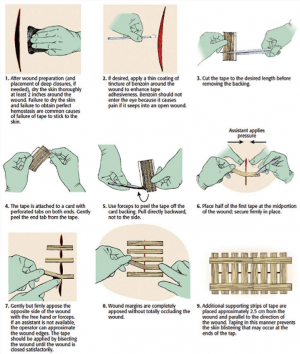
Steri-Strips
Skin Glue
- Useful for areas of low tension and well approximated wounds
- Apply 3 layers allowing 30 seconds for first layer to dry
- Avoid in bite wounds, contaminated wounds, puncture wounds, mucosal surfaces, areas of high moisture (groin, axilla)
- Avoid antibiotic ointments which can prematurely dissolve glue
Scalp Laceration
- Scalp laceration can be done with staples or if the patient has enough hair with Hair Apposition Technique by twisting hair together and using dermabond.
- Can bleed a lot, consider figure of 8 stitch to help with hemostasis
- Often accompanied by hematomas which may require evacuation for proper skin alignment
Aftercare
- Consider antibiotics for
- Wounds contaminated by debris or feces
- Caused by punctures or bites
- Tissue destruction or in avascular areas
- Neglected wounds
Wounds contaminated by fresh water and plantar puncture wounds through athletic shoes should include Pseudomonas coverage
- Splinting
- Wounds over flexor surfaces or tension
- Tetanus prophylaxis
- Tdap 0.5cc IM to patients >7y with no booster within 5 yr
- Hypertet 250 u IM at diff site from Tdap if NO history of Td or < 3 doses given
- Require follow up Tdap at 1mo & 1 yr; age>60 = high risk of poor immunization
- Dressing
- Keep moist, not wet
- Bandaid, xeroform, or ointment
- Keep moist, not wet
- Wound check
- 48-72 hrs ONLY if high risk wound
- No point in checking before 48hr (takes this long for infection to occur)
- 48-72 hrs ONLY if high risk wound
Scar Minimization
- Preventing infection
- Keep wound clean and covered
- Apply antibiotic ointment twice daily
- Once healed, encourage daily sunscreen use and Vitamin E creams
When to Call a Consultant
- Signs of neurovascular or tendon injury
- Facial wounds that cross cosmetic boundaries
- Tissue loss
Billing
- Anatomical location of wound
- Size of wound
- Length (cm) <2.5, 2.6-5.0, 5.1-7.5, 7.6-12.5, 12.5-20.0, 20.1-30.0, >30.0
- Complexity
- Simple, intermediate, or complex (depends on debridement, layers, complex stitch, drain, etc.)
- Type and number of sutures
See Also
- Soft Tissue Foreign Body
- Sutures
- Lip Laceration
- Fingertip Laceration
- Eyelid Laceration
- Tongue Laceration
- Nailbed laceration
- Conjunctival laceration
- Bites
- LET
References
- Moscati RM, Mayrose J, Reardon RF, Janicke DM, Jehle DV. A multicenter comparison of tap water versus sterile saline for wound irrigation. Acad Emerg Med. 2007 May;14(5):404-9
- Weiss EA, Oldham G, Lin M, Foster T, Quinn JV. Water is a safe and effective alternative to sterile normal saline for wound irrigation prior to suturing: a prospective, double-blind, randomised, controlled clinical trial. BMJ Open. 2013 Jan 16;3(1).
- Fernandez R, Griffiths R. Water for wound cleansing. Cochrane Database Syst Rev. 2012 Feb 15;(2):CD003861.
- Moscati RM, Reardon RF, Lerner EB, Mayrose J. Wound irrigation with tap water. Acad Emerg Med. 1998 Nov;5(11):1076-80.
- KUNDU S, et. al. Principles of Office Anesthesia: Part II. Topical Anesthesia Am Fam Physician. 2002 Jul 1;66(1):99-102.
- Esmailian M, Azizkhani R, Jangjoo A, Nasr M, Nemati S. Comparison of Wound Tape and Suture Wounds on Traumatic Wounds' Scar. Adv Biomed Res. 2018;7:49. Published 2018 Mar 27. doi:10.4103/abr.abr_148_16
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.