Juvenile nasopharyngeal angiofibroma
Background
- Juvenile nasopharyngeal angiofibromas (JNAs) are rare, highly vascular and aggressive tumors that almost exclusively present in adolescent males[1]
- Primary vascular supply in almost all tumors arise from the internal maxillary artery, and some patients may present primarily with recurrent and poorly controlled epistaxis[2]
Clinical Features

- Adolescent males most common
- Almost always unilateral
- Often presenting with history consistent with sinusitis, though with abnormal elements that may include cranial nerve abnormalities, or failure of treatment
- Can present with asymmetric facial swelling/pain
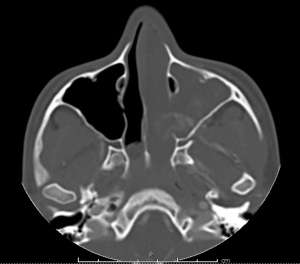
- Tumors can lead to local destruction and invasion, and can extend through ethmoid plate and cause cranial nerve deficits, decreased visual acuity, and abnormal extraocular movements
- Almost all are primarily in nasopharynx, but extranasal cases have been reported
- Highly prone to epistaxis
Differential Diagnosis
Rhinorrhea
- Upper respiratory infection, influenza
- Sinusitis
- Juvenile nasopharyngeal angiofibroma
- Nasal polyposis
- Nasal mass
- Nasal foreign body
- CSF leak (e.g. basilar skull fracture)
- Toxic inhalation (e.g. selenium toxicity, neurotoxic shellfish poisoning)
Evaluation
- In conjunction with consultants, will need MRI preferably, CT if unavailable
- Thorough evaluation of CN I-XII, with emphasis on smell, visual acuity, extraocular movements
Management
- Urgent ENT consultation for surgical planning
- Though some cases will resolve later in life, management is generally surgical with prior embolization[3]
- If uncontrolled bleeding, follow standard epistaxis treatments and contact IR for possible embolization
Disposition
- Discharge with ENT follow up
- Strict no digital trauma to nose, no foreign bodies, no steroid inhalers-avoid anything that would increase bleeding risk
- If cranial nerve involvement may consider admission for observation prior to urgent surgery
See Also
External Links
References
- Mehan, R., Rupa, V., Lukka, V. K., Ahmed, M., Moses, V., & Shyam Kumar, N. K. (2016). Association between vascular supply, stage and tumour size of juvenile nasopharyngeal angiofibroma. European Archives of Oto-Rhino-Laryngology, 273(12), 4295–4303. https://doi.org/10.1007/s00405-016-4136-9
- Mishra, A., Verma, V., & Mishra, S. C. (2017). Juvenile ‘Perinasal’ Angiofibroma. Indian Journal of Otolaryngology and Head & Neck Surgery, 69(1), 67–71.
- Mishra, A., & Verma, V. (2019). Implication of embolization in residual disease in lateral extension of juvenile nasopharyngeal angiofibroma. Journal of Oral Biology and Craniofacial Research, 9(1), 115–118.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.