Inferior shoulder dislocation
Background

Inferior dislocation with fracture of the greater tuberosity. Note how the humerus is abducted.
- Also known as "Luxatio Erecta" due to the affected arm being held 'erect', in a fully-abducted position
- About 0.5% of shoulder dislocations[1]
- Typically caused by hyperabduction
- Levers the humeral neck against the acromion
- Rarely caused by high-energy force applied to shoulder from above[2]
- Frequently associated with significant soft tissue injury or fracture[1]
Clinical Features
- Humerus fully abducted
- Hand on or behind head
- Humeral head palpable in axilla or lateral chest wall[1]
Differential Diagnosis
Shoulder and Upper Arm Diagnoses
Traumatic/Acute:
- Shoulder Dislocation
- Clavicle fracture
- Humerus fracture
- Scapula fracture
- Acromioclavicular injury
- Glenohumeral instability
- Rotator cuff tear
- Biceps tendon rupture
- Triceps tendon rupture
- Septic joint
Nontraumatic/Chronic:
- Rotator cuff tear
- Impingement syndrome
- Calcific tendinitis
- Adhesive capsulitis
- Biceps tendinitis
- Subacromial bursitis
Refered pain & non-orthopedic causes:
- Referred pain from
- Neck
- Diaphragm (e.g. gallbladder disease)
- Brachial plexus injury
- Axillary artery thrombosis
- Thoracic outlet syndrome
- Subclavian steal syndrome
- Pancoast tumor
- Myocardial infarction
- Pneumonia
- Pulmonary embolism
Evaluation
- Plain film X-ray in at least 2 views
Management
- Closed reduction
- Consider procedural sedation
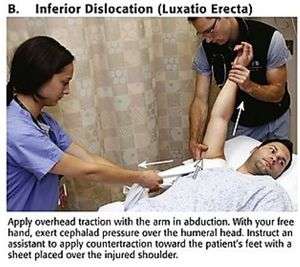
Single-Step Technique[3]
- Place sheet over upper shoulder and chest wall
- Have assistant grasp sheet and provide countertraction
- Grasp arm and apply traction upward and outward (along humeral axis)
- Place arm in shoulder immobilizer
- Obtain post-reduction radiographs
Two-Step Technique[4] [5]
- Converts inferior dislocation to anterior dislocation to allow reduction
- Place one hand on the lateral mid-shaft of the humerus
- Place second hand on medial epicondyle of elbow
- Use first hand to apply pressure to the mid-shaft of the humerus while the second hand pulls the elbow cephalad
- Perform reduction of the anterior shoulder dislocaiton
- Place arm in shoulder immobilizer
- Obtain post-reduction radiographs
- Failure of closed reduction may occur secondary to "buttonholing" of humeral through defect in glenohumeral capsule → consult ortho for open reduction[6]
Contraindications to closed reduction[1]
- Humeral neck or shaft fracture
- Suspected major vascular injury
- In these cases, open reduction is indicated
Complications
- Axillary nerve palsy in 60% (usually rapidly resolves after reduction[2]
- Humerus fracture in 37%
- Rotator cuff tear in 12%
Disposition
- Discharge after successful reduction
- Outpatient orthopedic surgery follow-up
See Also
References
- Imerci A, Gölcük Y, Uğur SG, et al. Inferior glenohumeral dislocation (luxatio erecta humeri): report of six cases and review of the literature. Ulus Travma Acil Cerrahi Derg. 2013 Jan;19(1):41-4.
- Grate I Jr. Luxatio erecta: a rarely seen, but often missed shoulder dislocation. Am J Emerg Med. 2000 May;18(3):317-21.
- Amanda E. Horn and Jacob W. Ufberg. Management of Common Dislocations. http://clinicalgate.com/management-of-common-dislocations/
- Davenport M. Procedures for orthopedic emergencies. In: Bond M, ed. Orthopedic Emergencies: Expert Management for the Emergency Physician. Cambridge: Cambridge University Press; October 31, 2013.
- Horn A. Management of Common Dislocations. In: Roberts and Hedges' Clinical Procedures in Emergency Medicine. 6th ed. Philadelphia, PA: Elsevier; 2014.
- Lam AC, Shih RD. Luxatio Erecta Complicated By Anterior Shoulder Dislocation During Reduction. Western Journal of Emergency Medicine. 2010;11(1):28-30.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.