Incarcerated uterus
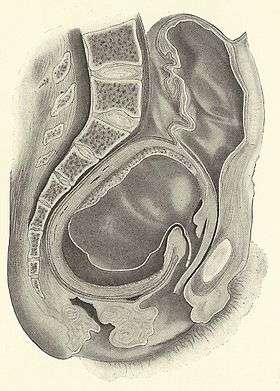
Incarcerated Uterus: Compression and anterior displacement of bladder into abdominal cavity with compression of rectum. Most common presenting symptoms is urinary retention.
Background
- Retroverted uterus is a normal variant (up to 20% of the population).
- During pregnancy, a retroverted uterus spontaneously flips to become anteverted at 14-16 weeks gestation age.
- Incarcerated uterus = impregnated retroverted uterus that is unable to spontaneously revert because the fundus is wedged below the sacral promontory.
- Growth of uterus during pregnancy in retroverted position leads to compression of pelvic organs leading to symptomatology.
Clinical Features
History
- Occurs only during pregnancy
- Symptomatology is the result of compression of pelvic structures from enlarging uterus
- Urinary Symptoms
- Urinary retention is the most common presenting symptom.
- Overflow incontinence
- Urgency, frequency
- Dysuria
- Rectal symptoms
- Constipation
- Rectal pressure, tenesmus
- Uncontrollable lower abdominal pain
- Pelvic pain
- Back pain
- Vaginal Bleeding
PMH
- Posterior and/or fundal fibroids
- Endometriosis, adhesive disease (prior surgery, peritonitis, PID)
- Prior history of incarcerated uterus
Bimanual Exam
- ACOG Recommendation: All women with second trimester urinary retention should have a pelvic exam performed at presentation to exclude an incarcerated retroverted uterus
- Findings
- Extremely anterior cervix
- Cervix posterior to pubic symphysis
- Acutely angled vaginal canal
- Unable to palpate uterus through abdomen
Transvaginal Ultrasound
- Difficulty to identify cervix in 2nd and 3rd trimester
- Cervix extends upward, superior to the bladder and pubic symphysis
- Bladder will appear elongated and distended due to compression of uterus
Differential Diagnosis
<20 Weeks
- Ectopic pregnancy
- First trimester abortion
- Complete abortion
- Threatened abortion
- Inevitable abortion
- Incomplete abortion
- Missed abortion
- Septic abortion
- Round ligament stretching
- Incarcerated uterus
- Malposition of the uterus
>20 Weeks
- Labor/Preterm labor
- Placental abruption
- Placenta previa
- Vasa previa
- Uterine rupture
- Vaginal trauma
- HELLP syndrome
- Cholestasis of pregnancy
- Chorioamnionitis
- Incarcerated uterus
- Acute fatty liver of pregnancy
- Malposition of the uterus
- Placenta accreta
- Placenta increta
- Placenta percreta
Urinary retention
- Obstructive causes
- BPH
- Prostate cancer
- Blood clot
- Urethral Stricture
- Bladder Calculi
- Bladder neoplasm
- Foreign body, urethral or bladder
- Ovarian/uterine tumor
- Incarcerated uterus
- Neurogenic causes
- Multiple sclerosis
- Parkinson's
- Brain tumor
- Cerebral vascular disease
- Cauda equina syndrome
- Spinal cord compression (non-traumatic)
- Intervertebral disk herniation
- Neuropathy
- Nerve injury from pelvic surgery
- Postoperative retention
- Trauma
- Urethral injury
- Bladder injury
- Spinal cord injury
- Extraurinary causes
- Perirectal or pelvic abscesses
- Rectal or retroperitoneal masses
- Fecal impaction
- Abdominal Aortic Aneurysm
- Psychogenic causes
- Psychosexual stress
- Acute anxiety
- Infection
- Cystitis
- Prostatitis
- Herpes Simplex (genital)
- Herpes Zoster involving pelvic region
- Local Abscess
- PID
- Meds
- Anticholinergics
- Antihistamines
- Cold meds
- Sympathomimetics
- TCA
- Muscle relaxants
- Opioids
Evaluation
- ABC’s and Resuscitation if necessary
- 2 large bore IVs
Labs
- Urine pregnancy, beta-HCG
- CBC with differential
- BMP, Mg/Phos, LFTs
- UA/Urine Culture
- PTT/PT/INR
- Type and cross 2 units PRBC if bleeding concern
Imaging
- Transvaginal Ultrasound
- Non-emergent MRI if unable to obtain transvaginal ultrasound
- Consider post-void residual
Management
- Consultation with OB/GYN upon diagnosis
Reduction of Incarcerated Uterus (ACOG Recommendations, 2014)
- Bladder decompression
- Insertion of indwelling Foley Catheter
- Pelvic exam to confirm diagnosis
- Acute anterior angulation of vagina
- Cervix positioned behind the pubic symphysis
- Fundus not palpable abdominally
Next steps are performed to achieve reduction of uterus by external/internal manipulation and should be performed with OB/GYN consultation
- Patient position
- Knee-chest or all fours
- Manual reduction
- Ensure bladder fully void
- Vaginal examination with or without anesthesia
- Colonoscopic
- Gas insufflation of colon under anesthesia
- Other
- Amnioreduction
- Surgical exploration through laparotomy
Delivery
- C-section
- Risk of uterine rupture if allowed to labor
Complications
- Maternal
- Acute renal failure
- Severe hypertension resistant to medications
- Lower limb edema
- Uterine ischemia
- Sepsis
- DVT, Post-partum PE
- Fetal
- Premature labor
- Fetal mortality rate 33% (Gibbons and Paley)
Disposition
- Admit
- From the limited number of case studies, it appears most patients were admitted for inability to void, pain control, reduction of incarcerated uterus.
See Also
External Links
References
- Newell S, Crofts J, Grant S. The Incarcerated Gravid Uterus Complications and Lessons Learned. American College of Obstetricians and Gynecologist 2014, 123:423-427
- Gardner C, Jaffe T, Hertzberg B, Javan R, Ho L. The Incarcerated Uterus: A review of MRI and Ultrasound Imaging Appearances. American Journal of Roentgenology. 2013;201: 223-229.
- Gibbons JM Jr, Paley WB. The incarcerated gravid uterus. Obstet Gynecol 1969; 33:842–845
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.