Internuclear ophthalmoplegia
Background
- Focal neuro deficit caused by injury or dysfunction of medial longitudinal fasciculus
- Paramedian Pontine Reticular Formation (PPRF) is the conjugate gaze center for horizontal eye movements. Innervates ipsilateral Abducens (CN VI) nucleus. Abducens nucleus signals ipsilateral lateral rectus to contract and sends a second via MLF to contralateral oculomotor (CN III) nucleus, causing contraction on the contralateral medial rectus.
- Associated with one and one-half syndrome (lesion involving the PPRF and ipsilateral MLF)
Clinical Features
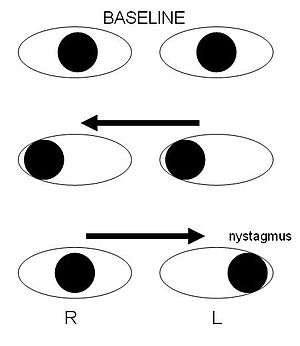
Schematic of right internuclear ophthalmoplegia caused by injury to right medial longitudinal fasciculus
Differential Diagnosis
- Multiple sclerosis (most common cause in young patients)
- Stroke
- Malignancy located in brainstem and 4th ventricle
- CN III palsy would show additional deficit including weakness of elevation, ptosis, pupil dilation
Evaluation
- Evaluate for underlying cause based on clinical presentation
- The use of optokinetic tape is highly sensitive for testing for INO
- MRI
Management
- Treat underlying condition
- Symptoms will often resolve on their own. Patients with cerebrovascular disease are less likely to have recovery.
- Patching of eye can aid in relief of diplopia
- Diframpadine, potassium channel blocker, has been used in patients with demyelinating disease
Disposition
See Also
External Links
References
Ropper A, Klein J, Samuels M. Adams and Victor's Principles of Neurology 10th Edition. McGraw-Hill Education / Medical; 2014.
Serra A, Skelly MM, Jacobs JB, et al. Improvement of internuclear ophthalmoparesis in multiple sclerosis with dalfampridine. Neurology 2014; 83:192.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.