Hypothermia
Background
Definition: Core Temperature <35°C (95°F)
- Unintentional hypothermia (core cooling <35°C) is associated with significant morbidity and mortality. Roughly 1500 persons die of accidental hypothermia in the US annually.[1]
- Despite the high mortality associated with pre-hospital arrest, well-directed treatment can result in complete neurologic recovery in the hypothermic patient.[2]
- 50% who die of hypothermia are >65 years old[3]
- Risk of cardiac arrest increased with temperature <32°C, as stable cardiac rhythms can quickly degenerate into unstable rhythms. Hypothermic patient without a pulse must be managed differently due to physiology changes that occur at low temperatures. Defibrillation and many medications may be ineffective until the core temperature is above 30.0°C. If defibrillation is warranted but unsuccessful, active rewarming should be initiated while CPR is continued.
Causes of Hypothermia
- Increased heat loss
- Environmental exposure
- Avalanche victims
- Homeless population
- Elderly patients → particularly low income during winter months
- Submersion injuries
- Induced vasodilation
- Environmental exposure
- Decreased heat production
- Endocrine
- Hypopituitarism
- Hypothyroidism
- Hypoadrenalism
- Hypoglycemia
- Neuromuscular inefficiency
- Extremes of age
- Impaired shivering
- Erythrodermas
- Psoriasis
- Exfoliative dermatitis
- Ichthyosis
- Eczema
- Burns
- Impaired Thermoregulation
- Other
- Endocrine
Clinical Features
Swiss Hypothermia Staging System[4]
| Classification | Temperature | Signs/Symptoms |
|---|---|---|
| I / Mild | 32-35°C (90-95°F) | Shivering, awake |
| II / Moderate | 28-32°C (82-90°F) | Shivering, depressed mental status |
| III / Severe | 20-28°C (68-82°F) | unconscious/severely depressed mental status, shivering ceases |
| IV / Profound | <20°C (68°F) | unobtainable VS |
Complications
- Acid-base disorders
- "Afterdrop"
- Initial drop in temperature and MAP as rewarming is started due to loss of vasoconstriction/AV shunting colder peripheral tissues
- Aspiration pneumonia
- Bleeding
- Decreased platelet function and inhibition of coagulation cascade
- Cold injuries
- Dysrhythmias
- Disseminated Intravascular Coagulation
- Hypothermia induced coagulopathy
- Pancreatitis
- Rhabdomyolysis
- Thromboembolism
- Secondary to hemoconcentration, increased blood viscosity, and poor circulation
- Ineffective Drugs
- Protein binding increases as body temperature drops, and most drugs become ineffective
- Pharmacologic manipulation of the pulse and blood pressure generally should be avoided
- Oral meds poorly absorbed because of decreased gastrointestinal motility
- Intramuscular route avoided due to poor absorption from vasoconstricted sites
Differential Diagnosis
Evaluation
- Use low-reading thermometer
- Some standard thermometers record only to 34°C
- Measure core temperature with esophageal probe if intubated (most accurate)
- Check blood glucose as can be very high in DM or CVA or low when metabolized to keep warm
- Potassium >10-12 mEq/L not compatible with life
- Coagulopathy: clotting factor activity and platelet function significantly reduced at temperature < 34°C
- Blood is rewarmed for lab testing so results may appear normal
- If ABG is rewarmed before analysis, results will be different from patient's actual acid/base state
- Refer to therapeutic hypothermia for over and underestimations
ECG
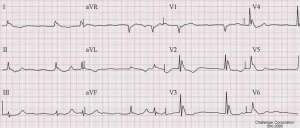
Atrial fibrillation and Osborn J waves in a person with hypothermia.
- Typical sequence is sinus bradycardia → atrial fibrillation with slow ventricular response → ventricular fibrillation → asystole
- Other ECG findings:
- Osborn (J) wave - Size of wave correlates with degree of hypothermia. No prognostic value.
- Muscle tremor artifact
- T-wave inversions
- PR, QRS, QT prolongation
- ST segment elevation or depression
- AV block
- PVCs
General Management
Handling
- Handle patient gently
- V-fib may be induced by rough handling of patient due to irritable myocardium (anecdotal)
O2
- Hypothermia causes leftward shift of oxyhemoglobin dissociation curve
- Intubation
- Intubate gently
- if RSI is given medications may act at a slower rate
IVF
- Patients are also hypovolemic since hypothermia causes impaired renal concentrating ability, in turn causing cold diuresis
- Patients are prone to rhabdomyolysis and will need hydration
- Intravascular volume is lost due to extravascular shift
- NS preferred over LR as cold liver poorly metabolizes LR
CPR
- Only perform if patient truly does not have a pulse (unnecessary CPR may lead to V-fib)
- Spend 30-45s attempting to detect respiratory activity and pulse before starting CPR
Dysrhythmias
- May occur spontaneously if temperature <30°C (86°F)
- Rewarming is treatment of choice
- Most dysrhythmias (e.g. sinus brady, a-fib/flutter) require no other therapy
- Activity of antiarrhythmics is unpredictable in hypothermia
- Hypothermic heart is relatively resistant to atropine, pacing, and countershock
- Ventricular tachycardia or Ventricular fibrillation are most common
Antibiotics
- Give if suspect sepsis (e.g. hypothermia fails to correct with rewarming measures)
Thiamine
- Consider if Wernicke disease is possible cause of hypothermia (e.g. alcoholic patient)
Hydrocortisone
- Consider if patient has history of adrenal suppression or insufficiency
- 100mg Hydrocortisone
Levothyroxine
- Consider if any suspicion for hypothyroidism/myxedema coma
- Could cause dysrhythmia or cardiac ischemia if not in myxedema coma
Hyperglycemia
- Hyperglycemia common in hypothermia:
- Stimulates catecholamine induced glycogenolysis
- Inhibits insulin release and uptake by cell membranes
- Rebound hypoglycemia during rewarming can occur if clinicians too aggressively deliver exogenous insulin
Rewarming
Recommendations on Rewarming Modality based on Temperature and Clinical picture
| Stage of Hypothermia | Recommended rewarming modality |
| I/ Mild: 32-35°C (90-95°F) | Passive external |
| II/ Moderate: 28-32°C (82-90°F) | Active external |
| III/ Severe: 20-28°C (68-82°F) | Active internal |
| IV/ Profound: <20°C (68°F) | As severe + modified ACLS |
Passive External
- Prevent additional losses → remove wet clothes
- Heated room
- Blankets - If patient still shivering, capable of rewarming 0.5°C/hr
Active External
- Rewarm trunk BEFORE the extremities, otherwise you cause further hypotension ("core temperature afterdrop")
- Afterdrop: warmed vasodilated peripheral tissue allows cooler blood in extremities to circulate back to core
- Options:
- Warm water immersion (Capable of 2-4°C/Hr rewarming)
- Heating blankets
- Radiant heat
- Forced air - e.g. Bair hugger (Up to 1-2.5°C/Hr rewarming)
- Warm humidified air via facemask or endotracheal tube
Active Internal
Options:
- Heated IV fluids: 38-42°C.
- GI tract lavage
- Can cause fluid and electrolyte fluctuations, also risk of pulmonary aspiration
- Bladder lavage
- Small surface area available for heat exchange
- Thoracic lavage
- Peritoneal lavage
- Bypass/ECMO[8]/AV Dialysis
Rewarming Rates
| Mode | °C/Hr | Comments |
| Passive External | ||
| Shivering[9] | 1.5 | |
| Warming Blanket[9] | 2 | |
| Active External | ||
| Warm IV fluids (47°C) | 1-3 | Highly variable; Limited by tubing distance, requires large volumes with risk of volume overload |
| Forced air (Bair hugger) | 1-2.5 | |
| Warm water immersion | 2-4 | |
| Active Internal | ||
| Warm Humidified Air (intubated) | 0.5-1.2 | Low heat transport capacity |
| Peritoneal Lavage[9] | 3 | |
| Thoracic Lavage[9] | 3-6 | |
| Hemodialysis[9] | 3-4 | |
| Open thoracotomy lavage | Up to 8 (median 3) | Highly invasive. 71% survival in 1 study |
| Cardiac Bypass[9] | 7-10 |
Management of the coding hypothermic patient
- Rhythms can quickly degenerate into unstable rhythms
- Be careful when inserting guidewires, persistent shocks can degenerate fib into asystole
- Standard ACLS guidelines may not apply:
- Any organized rhythm should be assumed to be perfusing the patient adequately
- Starting CPR may precipitate fatal ventricular rhythms
- Modified vs. Standard ACLS:
- ERC recommends up to 3 defibrillations with [[epi] held until temperature >30°C, then epinephrine interval of 6 min until temperature >35°C
- AHA recommends 3 defibrillations and 3 rounds of epinephrine with further dosing guided by clinical response
- Recent consensus suggest only one defibrillation and round of ACLS meds → rewarm 5°C → one defib/meds → Repeat
Disposition
- ICU for severe cases
External Links
References
- Baumgartner EA, Belson M, Rubin C, Patel M. Hypothermiaand other cold-related morbidity emergency department visits: United States, 1995-2004. Wilderness Environ Med 2008;19:233-237
- Friberg H, Rundgren. Submersion, accidental hypothermia, and cardiac arrest, mechanical chest compressions as a bridge to final treatment: a case report. Scand J Trauma Resusc Emerg Med. 2009; 17: 7
- Centers for Disease Control and Prevention: Hypothermia-related deaths—United States, 2003–2004. MMWR Morb Mortal Wkly Rep 54: 173, 2005
- Brown et al., Accidental Hypothermia. N Engl J Med 2012; 367:1930-1938
- Hoek T. 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010. 122:5829-5861
- Fildes J, Sheaff C, and Barrett J. Very hot intravenous fluid in the treatment of hypothermia. J Trauma. 1993; 35(5):683-686.
- Sheaff CM, Fildes JJ, Keogh P, et al. Safety of 65 degrees C intravenous fluid for the treatment of hypothermia. Am J Surg. 1996; 172(1):52-55.
- Ginty C, et al. Extracorporeal membrane oxygenation rewarming in the ED: an opportunity for success. American Journal of Emergency Medicine. 2014 December 3 (ahead of print).
- Kempainen, R. R. and Brunette, D. D. The Evaluation and Management of Accidental Hypothermia. Respir.Care 2004;49(2):192-205
- Schaller M, Fischer AP, Perret CH. Hyperkalemia: A Prognostic Factor During Acute Severe Hypothermia. JAMA. 1990;264(14):1842–1845. doi:10.1001/jama.1990.03450140064035
- Paal P, Gordon L, Strapazzon G, et al. Accidental hypothermia-an update : The content of this review is endorsed by the International Commission for Mountain Emergency Medicine (ICAR MEDCOM). Scand J Trauma Resusc Emerg Med. 2016;24(1):111. Published 2016 Sep 15. doi:10.1186/s13049-016-0303-7
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.