Hypokalemia
Background
Clinical Features
- Central nervous system
- Gastrointestinal
- Renal
- Cardiovascular
Differential Diagnosis
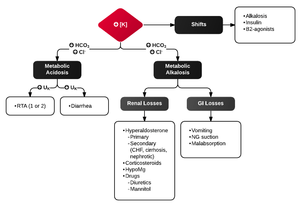
Differential diagnosis of hypokalemia
Intracellular Shift
- Alkalosis (each 0.10 rise in pH causes 0.5 decrease)
- Insulin
- Beta agonists
- Hypokalemic periodic paralysis
Decreased intake
- Special diets or those low in potassium
- Chronic alcohol abuse
Increased loss
- GI
- Renal
- Diuretics
- Hyperaldosteronism
- Exercise
- Hypercalcemia
- Hypomagnesemia
Drugs
- Penicillins
- Lithium
- L-dopa
- Theophylline, methylxanthines (e.g. caffeine
- Insulin
- Barium
- Quinine
- Catecholamines
Evaluation
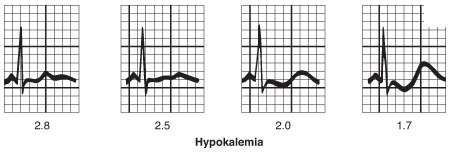
- Serum potassium level is diagnostic
- Normal = 3.5-5meq/L
- Severe hypokalemia = <2.5meq/L
- Always check magnesium
- Suggestive ECG findings:
Management
- Potassium repletion (PO or IV)
- Every 10mEq KCl → serum K ↑ ~0.1mEq/L
- PO preferred (if symptomatic or level is <2.5, both oral and IV should be given)
- Oral potassium
- Inexpensive and rapidly absorbed
- KCl tablet (elixir form available but has poor taste)
- K-Dur (extended release tablet) is large and may be difficult to swallow
- If sending patient home can also increase food intake of potassium as an alternative or supplementing potassium tablets. Printable table that can be given to the patient available at this reference: [1].
- Intravenous potassium
- Must be given in dilute solutions at slow rate (10meq/hour) to minimize side effects and cardiac toxicity
- Generally should not give more than 40mEq via IV
- Side effects: Local tissue burning, phlebitis, sclerosis
- Also treat Hypomagnesemia if present
- Re-check ECG after treatment [2]
- Hypokalemia in acute or recent myocardial infarction places patients at much higher risk for ventricular fibrillation[3]
- Previous studies and many professional organizations recommend maintaining K between 4.0 - 5.0 mEq/L in MI patients
- However, more recent studies suggest 3.5 - 4.5 mEq/L results in the lowest mortality
Disposition
- Based on underlying cause
- One admission criteria is potassium less than 3.0 meq/L and a QTc that is close to or more than 500 msec. [4]
References
- Potassium Supplement (Oral Route, Parenteral Route) from Mayo Clinic
- Slovis, Corey. "Electrolyte Emergencies". Presentation.
- Goyal A et al. Serum Potassium Levels and Mortality in Acute Myocardial Infarction. JAMA. 2012;307(2):157-164.
- EM:RAP 2018 August Electrolyte Emergencies - Part 1 - All Things Potassium
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.