Hyperkalemia
Background
- Defined as >5.5 mEq/L
- Potassium secretion is proportional to flow rate and sodium delivery through distal nephron
- Thus, loop & thiazide diuretics cause hypokalmia
Medication Causes
Alter transmembrane potassium movement
- β blockers
- Digoxin
- Potassium-containing drugs
- Potassium supplements
- Salt substitutes
- Hyperosmolar solutions (mannitol, glucose)
- Suxamethonium
- Intravenous cationic amino acids
- Stored red blood cells (haemolysis releases potassium)
- Herbal medicines (such as alfalfa, dandelion, horsetail, milkweed, and nettle)
Reduce aldosterone secretion
Block aldosterone binding to mineralocorticoid receptors
- Spironolactone
- Eplerenone
- Drospirenone
- Potassium sparing diuretics (amiloride, triamterene)
- Trimethoprim
- Pentamidine
Clinical Features
Typically non-specific
Differential Diagnosis
Hyperkalemia
- Pseudohyperkalemia: hemolyzed specimen, prolonged tourniquet use prior to blood draw, thrombocytosis or leukocytosis
- Redistribution (shift from intracellular to extracellular space)
- Acidemia (see DKA)
- Cellular breakdown: see Rhabdomyolysis/Crush syndrome, electrical/thermal burn, hemolysis, see Tumor lysis syndrome
- Increased total body potassium
- Inadequate excretion: Acute/chronic renal failure, Addison's disease, type 4 RTA
- Drug-induced: potassium-sparing diuretic (spironolactone), angiotensin converting enzyme inhibitors (ACE-I), nonsteroidal anti-inflammatory drugs (NSAIDs)
- Excessive intake: diet, blood transfusion
- Other causes: succinylcholine, digitalis, beta-blockers
Peaked T-waves
- MI (hyperacute T waves)
- Hyperkalemia
- Benign Early Repolarization
- De Winter's T waves (acute LAD occlusion)
Wide-complex tachycardia
Assume any wide-complex tachycardia is ventricular tachycardia until proven otherwise (it is safer to incorrectly assume a ventricular dysrhythmia than supraventricular tachycardia with abberancy)
- Regular
- Monomorphic ventricular tachycardia
- PSVT with aberrant conduction:
- PSVT with bundle branch block^
- PSVT with accessory pathway
- Atrial flutter with bundle branch block^
- Sinus tachycardia with bundle branch block^
- Accelerated idioventricular rhythm (consider if less than or ~120 bpm)
- Metabolic
- Irregular
- Atrial fibrillation/atrial flutter with variable AV conduction AND bundle branch block^
- Atrial fibrillation/atrial flutter with variable AV conduction AND accessory pathway (e.g. WPW)
- Atrial fibrillation + hyperkalemia
- Polymorphic ventricular tachycardia
^Fixed or rate-related
Evaluation
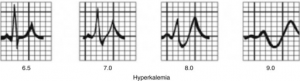
Diagrammatic representation of ECG changes with increasing hyperkalemia
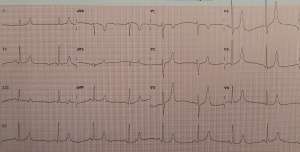
ECG in hyperkalemia with peaked T waves and small P waves
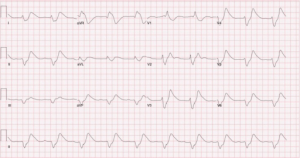
ECG with widened QRS complex and tall broad T waves
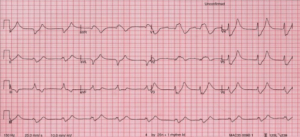
ECG showing sine wave pattern
Workup
ECG
Changes NOT always predictable and sequential
- 6.5 - 7.5 mEq/L: peaked T waves, prolonged PR interval, shortened QT interval
- 7.5 - 8.0 mEq/L: widened QRS interval, flattened P waves
- 10 - 12 mEq/L: sine wave, ventricular fibrillation, heart block
Diagnosis
- Based on lab testing (>5.5 mEq/L), although ECG may provide earlier information
- Consider pseudohyperkalemia (e.g. from hemolysis)
Management
Stabilize cardiac membranes
Indicated if there are any ECG changes or evidence of arrhythmias. Consider if K >7 mEq/L
- Either one of the following:
- Calcium gluconate: Give 10ml of a 10% solution over 10 mins
- Only 1/3 the calcium compared to calcium chloride
- Can cause hypotension due to osmotic shift
- Calcium chloride 1 gram IV
- Give over 1 - 2 minutes
- Extravasation is bad: use a good IV
- Usually given in code situations
- Calcium gluconate: Give 10ml of a 10% solution over 10 mins
- Takes effect in 15-30 minutes[1]
- (If given for hyperkalemic cardiac arrest, need to continue resuscitation for at least 30 minutes)
- Duration of action: 30 - 60 minutes [2]
- Use caution in patients taking Digoxin although risk of Stone heart may be unsubstantiated [3]
- Do serial ECGs to track progress: may need to give multiple doses
Shift K+ intracellularly
- Intravenous insulin + dextrose
- Give 10 units regular insulin intravenously with 25 to 50 grams (1 - 2 50 mL ampules) of 50% dextrose (D50)
- May withhold dextrose if blood sugar >300mg/dl (>17 mmol/L)
- Duration of effect: 4 - 6 hours
- Consider mixing in 10 cc NS syringe to ensure small volume of 10 units insulin fully administered via IV
- Insulin cleared renally, be careful about inducing hypoglycemia (ESRD patients).
- In a small 2017 retrospective cohort study, researchers found that giving 5 units of insulin instead of 10 units reduced serum potassium to the same extent as 10 units, with a lower rate of hypoglycemia.
- Consider decreasing to 5 units or increasing dextrose dose to 50g with following risk factors: pretreatment blood glucose <150, acute kidney injury/chronic kidney disease, no history of DM, weight <60kg, female sex [4]
- Give 10 units regular insulin intravenously with 25 to 50 grams (1 - 2 50 mL ampules) of 50% dextrose (D50)
- Nebulized albuterol 15 - 20mg
- Response is dose-dependent
- Peak effect: 30 minutes
- Duration of effect: 2 hours
- Sodium bicarbonate
- Generally not considered unless pH <7.1
- Pushing "ampules of hypertonic bicarbonate have been proven to be ineffective in RCTs"[5]
- For normovolemic or hypovolemic patients with metabolic acidosis:
- Give three amps of bicarbonate in a liter of D5W or sterile water
Remove K+ from body
- Intravenous furosemide (Lasix) 40 - 80mg
- Ensure adequate urine output first
- Decreases the potassium in three ways: dilution, shifting of potassium into muscle cells, and promotion of renal potassium excretion by alkalosis[6]
- More on how to use Lasix: IBCC Hyperkalemia Chapter
- Sodium polystyrene sulfonate (Kayexalate): 30 gm oral or per rectum
- Very Controversial, High Risk of Bowel Perforation, see: EBQ: Use of Kayexylate in Hyperkalemia
- Sodium zirconium cyclosilicate
- Potassium binder, similar to Kayexalate but without risk of bowel perforation[7]
- Intravenous lactated ringers solution for volume expansion if dehydrated, rhabdomyolysis, diabetic ketoacidosis or other acidosis (avoid NS, causes hyperchloremic acidosis which shifts potassium out of cells increasing level)
- consider isotonic bicarbonate if significant acidosis (D5W with 3 amps of bicarb per liter), can calculate bicarbonate deficit then divide by 150mEq/L to estimate number of liters of isotonic bicarbonate required) [8]
- Hydrocortisone if suspicious for adrenal insufficiency
- Definitive treatment is hemodialysis
Disposition
- Consideration for ICU for frequent electrolyte checks and close cardiac monitoring
External Links
References
- http://lifeinthefastlane.com/hyperkalemia/. Accessed 02/22/2016
- The Effect of Calcium on Severe Hyperkalemia http://hqmeded-ecg.blogspot.com/2015/04/the-effect-of-calcium-on-severe.html
- Erickson CP, Olson KR. Case files of the medical toxicology fellowship of the California poison control system-San Francisco: calcium plus digoxin-more taboo than toxic? J Med Toxicol. 2008 Mar;4(1):33-9
- Moussavi K1, Fitter S2, Gabrielson SW3, Koyfman A4, Long B5. Management of Hyperkalemia With Insulin and Glucose: Pearls for the Emergency Clinician. J Emerg Med. 2019 Jul;57(1):36-42.
- IBCC Hyperkalemia Chapter
- IBCC Hyperkalemia Chapter
- Beccari, Mario V, and Calvin J Meaney. “Clinical utility of patiromer, sodium zirconium cyclosilicate, and sodium polystyrene sulfonate for the treatment of hyperkalemia: an evidence-based review.” Core evidence vol. 12 11-24. 23 Mar. 2017, doi:10.2147/CE.S129555
- https://emcrit.org/pulmcrit/fluid-selection-using-ph-guided-resuscitation
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.