High altitude pulmonary edema
Background
- Also known as HAPE
- Noncardiogenic pulmonary edema due to increased microvascular pressure in the pulmonary circulation
- Hypoxic pulmonary vasoconstriction leads to pulmonary hypertension
- Most lethal of the altitude illnesses
- Occurs in <1/10,000 skiers in Colorado; 2-3% of Mt. McKinley climbers
- Typical patient is strong and fit; may not have symptoms of altered mental status before onset of HAPE
- Most commonly noticed on the second night at a new altitude
Risk Factors
- Heavy exertion
- Rapid ascent
- Cold
- Excessive salt ingestion
- Use of a sleeping medication
- Preexisting pulmonary hypertension
- Preexisting respiratory infection (children)
- Previous history of HAPE
Clinical Features
Early
Late
- Dyspnea at rest, marked weakness, productive cough, cyanosis, generalized rales
- Cough generates pink, frothy sputum
- Tachycardia and tachypnea correlate with severity of illness
- Altered mental status and coma (from severe hypoxemia)
Differential Diagnosis
Pulmonary Edema Types
Noncardiogenic pulmonary edema
- Negative pressure pulmonary edema
- Upper airway obstruction
- Reexpansion pulmonary edema
- Strangulation
- Neurogenic causes
- Iatrogenic fluid overload
- Multiple blood transfusions
- IV fluid
- Inhalation injury
- Pulmonary contusion
- Aspiration pneumonia and pneumonitis
- Other
- High altitude pulmonary edema
- Hypertensive emergency
- ARDS
- Sympathetic crashing acute pulmonary edema (SCAPE)
- Immersion pulmonary edema
- Hantavirus pulmonary syndrome
- Missed dialysis in kidney failure
Evaluation
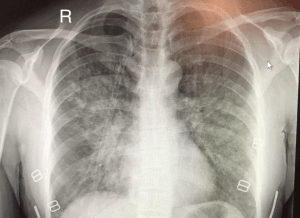
Chest x-ray of HAPE showing characteristic patchy alveolar infiltrates with right middle lobe predominance.
Workup
- ECG - right strain pattern
- CXR - Progresses from interstitial → localized-alveolar → generalized-alveolar infiltrates
- ABG - Hypoxemia with respiratory alkalosis
Evaluation
- Clinical diagnosis
Management
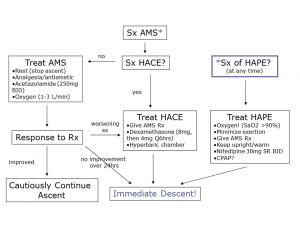
High altitude management algorithm.
- Immediate descent is treatment of choice - minimize exertion
- If cannot descend use combination of:
- Supplemental O2 - An oxygen concentrator is often used at high altitude ski resorts after the patient is titrated down to nasal cannula. A portable oxygen tank is used for ambulation. Can completely resolve the pulmonary edema within 36-72hr
- Hyperbaric bag - (e.g. Gamow Bag). Should not delay descent, if possible.
- Keep patient warm (cold stress elevates pulmonary artery pressure)
- Use expiratory positive airway pressure mask
- Nifedipine 30mg ER q12hr (or 20mg normal-release q8hr)[2]
- May consider the other medications listed below that are usually used for prevention
Disposition
- Admission
- Warranted for severe illness that does not respond immediately to descent
- Discharge
- Progressive clinical and X-ray improvement and a PaO2 of 60mmHg or SaO2>90%
- May re-ascend in 2-3 days if mild-moderate symptoms resolved that only required descent as the intervention
Prevention
- Nifedipine 20mg q8hr or 30mg ER q12hr while ascending is effective prophylaxis in patients with prior episodes of HAPE
- Tadalafil 10mg BID 24hr prior to ascent OR Sildenafil 50mg q8hr
- Salmeterol 125 mcg inhaled BID
- Acetazolamide 125mg BID for prevention of hypoxia
See Also
References
- Gallagher, MD, Scott A.; Hackett, MD, Peter (August 28, 2018). "High altitude pulmonary edema". UpToDate. Retrieved May 2, 2019.
- Luks AM, McIntosh SE, Grissom CK, et al. Wilderness Medical Society Practice Guidelines for the Prevention and Treatment of Acute Altitude Illness: 2014 Update. Wilderness & Environmental Medicine. 2014(25): S4–S14)
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.