High altitude cerebral edema
Background
- Also known as HACE
- Progressive neurologic deterioration in someone with acute mountain sickness or HAPE (due to ↑ ICP)
- Almost never occurs at <8,000ft
Clinical Features
- Altered mental status, ataxia, gait disturbance, stupor (most sensitive findings)
- Progresses to coma if untreated
- Uncertain mechanism, presumed cause is hypoxia leading to cerebral edema
- Headache, nausea/vomiting (not always present)
- Focal neuro deficits may be seen (3rd/6th CN palsies)
- Seizures are rare
Differential Diagnosis
Evaluation

Head CT of HACE showing diffuse effacement of cerebral sulci and compression of ventricles.
- Typically a clinical diagnosis
Management
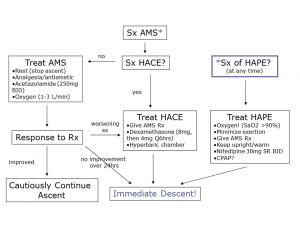
High altitude management algorithm.
- Immediate descent is the treatment of choice
- If descent not possible use combination of:
- Supplemental O2 (goal SpO2 90%)[2]
- Supportive hyperventilation
- Dexamethasone 8mg initially (PO, IM, or IV), then 4mg q6hr
- Acetazolamide 250mg BID (better as ppx)
- Hyperbaric bag (Gamow bag) if available
Prevention
- Acclimatization, slow ascent
- Acetazolamide 125mg BID (250mg BID if greater than 100kg)
- Dexamethasone 4mg q6h PO or IV
See Also
References
- Gallagher, MD, Scott A.; Hackett, MD, Peter (August 28, 2018). "High altitude pulmonary edema". UpToDate. Retrieved May 2, 2019.
- Hackett PH, Roach RC. High altitude cerebral edema. High Alt Med Biol 2004; 5:136-146.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.