Frostbite
Background
Whid chill chart
- Results from the freezing of tissue
- It is a disease of morbidity, not mortality
- Risk correlated with temperature and wind speed
- Risk is <5% when ambient temperature (includes wind chill) is > –15°C (5°F)
- Most often occurs at ambient temperature < –20°C (–4°F)
- Can develop within 2-3sec when metal surfaces that are at or below –15°C (5°F) are touched
- Most commonly affects distal part of extremities, face, nose, and ears
- High-risk groups: outdoor workers, elderly, homeless, drug or alcohol abusers, psychiatric disease
Pathophysiology
- Freezing alone is usually not sufficient to cause tissue death
- Thawing contributes markedly to the degree of injury
- Endothelial damage, beginning at the point of thaw, is the critical event in frostbite
- Resulting damage results in swelling, platelet aggregation, vessel thrombosis
Zones of Injury
- Zone of Coagulation
- Most severe and usually most distal
- Damage is irreversible
- Zone of Hyperemia
- Least severe and usually most proximal
- Generally recovers without treatment in <10d
- Zone of Stasis
- Middle zone characterized by severe, but possibly reversible, cell damage
- It is this zone for which treatment may have benefit
Clinical Features
Classification
Visual determination of tissue viability is difficult in first few weeks; classify early injuries as superficial or deep
| Degree | First (frostnip) | Second | Third | Fourth |
| Pathophys | Partial-skin freezing | Full-thickness skin freezing | Tissue loss involving entire thickness of skin | Extension into subcutaneous tissues, muscle, bone, and tendon; little edema |
| Symptoms | Stinging and burning, followed by throbbing | Numbness followed by aching and throbbing | Extremity feels like a "block of wood" followed by burning, throbbing, shooting pains | Deep, aching joint pain |
| Course | Numbness, erythema, swelling, dysesthesia, desquamation (days later) |
Substantial edema over 4-6 hours; skin blisters form within 6-24 hours; Desquamate and form hard black eschars over several days |
Hemorrhagic blisters form and are associated with skin necrosis and blue-gray discoloration | Skin is mottled with nonblanching cyanosis and formation of deep, dry, black eschar |
| Pain with rewarming | Minimal | Mild to moderate | Severe | None |
| Prognosis | Excellent | Good | Often poor | Extremely poor |
| Image |  |  |  |  |
Differential Diagnosis
Evaluation
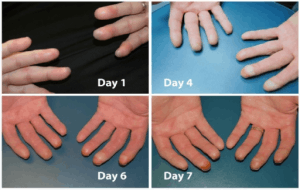
Second degree frostbite progression.
- Usually clinical
Management
- Thawing
- Do NOT attempt until the risk of refreezing is eliminated
- Refreezing will cause even more severe damage
- Rapid rewarming is the core of therapy and should be initiated as soon as possible
- Extremities
- Place in water with temperature of 40-42C (104-107.6)
- Approximately 20-30min, until extremity is pliable and erythematous
- OR consider 38-40°C in whirlpool bath with antibacterial soap[1]
- Face
- Apply moistened compresses soaked in warm water
- Extremities
- Do NOT attempt until the risk of refreezing is eliminated
- Analgesia
- Rewarming is very painful
- Provide parenteral opioids
- Local wound care
- Apply topical aloe vera cream q6hr (interrupts arachidonic acid cascade)
- Affected digits should be separated with cotton and wrapped with sterile, dry gauze
- Elevate involved extremities
- Blister removal is controversial
- Consider drainage of nonhemorrhagic bullae that interfere with movement
- Never debride hemorrhagic bullae
- Systemic care
- Tetanus
- Reported complication of frostbite; provide prophylaxis
- Antibiotics
- Controversial
- Penicillin G 500,000 units IV Q6 hours for 48-72 hours
- Topical bacitracin may be as good or better than IV penicillin
- Silver sulfadiazine cream not consistently beneficial
- May interact with aloe vera cream
- Surgery
- May be required if wet gangrene or infection occurs
- Usually not performed until full demarcation occurs (3-4wk)
Disposition
- Patients with superficial local frostbite may be discharged home if social circumstances allow
Complications
- Up to 65% of patients with frostbite experience sequelae from their injuries
- Hypersensitivity to cold, pain, ongoing numbness
- Arthritis, bone deformities, scars, and skin and nail dystrophia
See Also
Video
START_WIDGETcdad359bfbcd5f91-0END_WIDGET
References
- Crawford-Mechem C et al. Frostbite Treatment & Management. Aug 25, 2015. http://emedicine.medscape.com/article/926249-treatment#showall
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.