Facial paralysis
Background
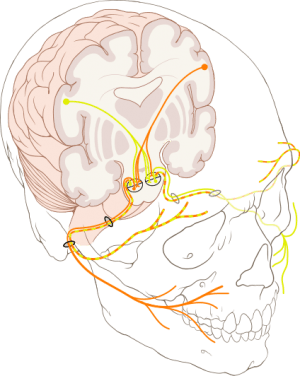
Bilateral course of facial nerve. Note that the forehead muscles receive innervation from both hemispheres of the brain, which is why there is forehead sparing for stroke but not Bell's palsy (or other peripheral facial nerve injury).
- Key to distinguish between central and peripheral facial nerve palsy
Causes
- Central
- Peripheral
- Idiopathic (Bell's palsy)
- Lyme disease
- Varicella-zoster
- HSV
- Facial trauma
Clinical Features

A person attempting to show his teeth and raise his eyebrows with Bell's palsy on his right side; notice how the forehead is NOT spared).

Patient with stroke (forehead sparing).
Central Process
- Forehead "sparing" or normal muscle tone of the forehead
Peripheral Process
- Weakness of forehead muscles
Central and Peripheral
- Unable to close eye
- Loss of nasolabial fold
- Asymmetric smile
Differential Diagnosis
Facial paralysis
- Bell's Palsy
- CVA
- Trigeminal neuralgia
- Tick paralysis
- Lyme Disease
- Herpes zoster oticus (Ramsay Hunt syndrome)
- CNS tumor
- Acoustic neuroma or other cerebellopontine angle lesions
- Meningioma
- Cerebellar pontine angle
- Facial nerve schwannoma
- Parotid
- Sarcoma
- Anesthesia nerve blocks
- Cerebral Aneurysms (vertebral, basilar, or carotid)
Evaluation
Central Process
Peripheral Process
- No labs or imaging routinely necessary
- Consider lyme serologies if endemic area
Management
Central Process
- Treat underlying pathology
Peripheral Process
- Prednisone (unless diagnosed Lyme disease)
- Empiric doxycycline if high suspicion for Lyme disease
- Consider valacyclovir for severe presentation if Lyme is negative
- Artificial tears
- Consider neurology follow-up
Disposition
See Also
External Links
References
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.