Dental avulsion
Background
- Dental emergency; for every minute that a permanent tooth remains out of the socket, the chance of successful reimplantation goes down by 1% [1]
- Tooth is completely removed from its socket
- Often associated with alveolar ridge fracture
Clinical Features
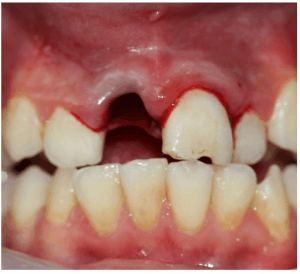
Avulsion of the right upper incisor.

Avulsed tooth
- Tooth missing from socket
- History of recent trauma
Differential Diagnosis
Evaluation
Work-up
- Consider facial films, abdominal films, or CXR if possibility of tooth aspiration or ingestion
Evaluation
- Determine when avulsion occurred and what storage solution used
- If re-implanting, best viability with immediate storage in Hank's Balanced Salt Solution, worst viability without any storage medium
- Account for all teeth
- Aspiration or swallowed
- Rule out fragments in lacerations/oropharyngeal space, or significant intrusive luxation/impaction
- Determine if tooth is primary or secondary
- Tetanus status
Management
Adult
- Replace avulsed tooth as soon as possible with local analgesia ± dental block (as long as no alveolar ridge fracture or severe socket injury)
- If reimplanted within 1hr 66% chance of good outcome
- Rinse (no scrubbing!) tooth in saline
- Manipulate tooth only by the crown (Avoid touching root to minimize damage to periodontal ligament)
- Splint tooth with adjacent teeth
- If extraoral time > 60 min, soak in citric acid/fluoride and consult dentist[2]
- Storage solution (in order of efficacy): Hank's Balanced Salt Solution > Milk > saliva > saline
- Doxycycline 100mg PO BID x 1week (helps periodontal ligaments heal)
- Penicillin OR Clindamycin are alternatives, especially in pediatrics
- Tetanus update
Child
Length of Periodontal Ligament Cell Viability Based On Storage Medium [5]
| Storage Medium | Length of Periodontal Ligament Viability |
| Dry (no storage medium) | < 60 minutes |
| Milk | 3 to 8 hours |
| Oral rehydration solution | 12 to 24 hours |
| Hanks’ balanced salt solution | 12 to 24 hours |
Disposition
- Discharge with dental follow-up on liquid diet
- Should be seen within 24-48 hours as splint only lasts up to 48 hours
See Also
- Dental Problems
References
- Amsterdam JT. Oral medicine. In: Marx JA, Hockberger RS, Walls RM, et al., eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 8th ed. St. Louis, MO: Mosby, Inc. 2014; (Ch) 70:895–908.
- Mayersak, RJ. Facial trauma, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 7. St. Louis, Mosby, Inc., 2010, (Ch) 42: 368-81.
- Amsterdam JT: Oral Medicine, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 7. St. Louis, Mosby, Inc., 2010, (Ch) 68:p 853-856
- Benko, K. Acute Dental Emergencies in EM. EM Practice. 2003, 5(5)
- Rosen’s Emergency Medicine: Concepts and Clinical Practice, 9th edition, Ron M. Walls, Robert S. Hockberger, Marianne Gausche-Hill, et al. Oral Medicine. Copyright 2017
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.