Croup
Background
- Also known as laryngotracheobronchitis
- Typically affects ages 6 mo-3 yr (peak in 2nd year)
- May affect older children
- Most common in fall & winter
Etiologies
- Parainfluenza (50% - 75%)
- Influenza A and B (usually more severe clinical picture)
- RSV
- Rhinovirus
- Consider Diphtheria if not immunized
- Spasmodic croup
- Sudden onset of barking cough/stridor
- No viral prodrome, unlike typical croup
- Difficult to differentiate from typical croup
- Must rule out foreign body
Clinical Features
- 1-3 days of URI symptoms, followed by barking cough, hoarse voice, and stridor
- Low-grade fever
- NO drooling or dysphagia
- Duration 4 - 7 days
- Usually most severe on days 3-4
Mild[1]
- 85% of cases
- Intermittent barking cough
- Stridor with agitation
- Mild tachypnea
- Mild tachycardia
Moderate[2]
- Fussy but alert, interactive, consolable by parents
- Stridor at rest
- Worsening stridor with agitation
- Increased work of breathing
Differential Diagnosis
- Allergic reaction
- Angioedema
- Asthma
- Bacterial tracheitis
- Congestive heart failure
- Croup
- Cystic fibrosis
- Diphtheria
- Epiglottitis
- Foreign body
- Inhalation injury
- Laryngeal fractures
- Laryngomalacia
- Mononucleosis and Epstein-Barr virus infection
- Peritonsillar abscess
- Pertusis
- Pneumonia
- Retropharyngeal abscess
- Subglottic stenosis
- Tracheomalacia
- Vascular ring
Pediatric stridor
- A minimal amount of edema or inflammation in the pediatric airway can result in significant obstruction
- Can lead to rapid decompensation
<6mo
- Laryngotracheomalacia
- Accounts for 60%
- Usually exacerbated by viral URI
- Dx w/ flexible fiberoptic laryngoscopy
- Vocal cord paralysis
- Stridor associated w/ feeding problems, hoarse voice, weak and/or changing cry
- May have cyanosis or apnea if bilateral (less common)
- Subglottic stenosis
- Congenital vs 2/2 prolonged intubation in premies
- Airway hemangioma
- Usually regresses by age 5
- Associated w/ skin hemangiomas in beard distribution
- Vascular ring/sling
>6mo
- Croup
- viral laryngotracheobronchitis
- 6 mo- 3 yr, peaks at 2 yrs
- Most severe on 3rd-4th day of illness
- Steeple sign not reliable- diagnose clinically
- Epiglottitis
- H flu type B
- Have higher suspicion in unvaccinated children
- Rapid onset sore throat, fever, drooling
- Difficult airway- call anesthesia/ ENT early
- H flu type B
- Bacterial tracheitis
- Rare but causes life-threatening obstruction
- Sx of croup + toxic-appearing = bacterial tracheitis
- Foreign body (sudden onset)
- Marked variation in quality or pattern of stridor
- Retropharyngeal abscess
- Fever, neck pain, dysphagia, muffled voice, drooling, neck stiffness/torticollis/extension
Evaluation
Work-up
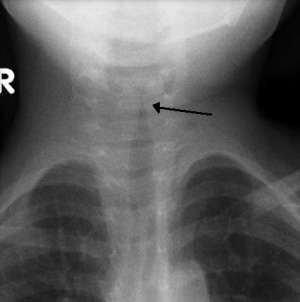
The steeple sign as seen on an AP neck X-ray (dedicated neck film not typically indicated).
- Consider CXR if concerned about alternative diagnosis
- In typical cases, imaging is not needed and does not change management
- Steeple sign on AP XR (not specific or sensitive)
- Consider nasal pharyngeal swab
Diagnosis
- Clinical
- Steeple sign unreliable
Westley Croup Score[4][5]
Helps to stratify patients into mild moderate and severe and guide treatment
| Feature | Number of points assigned for this feature | |||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | |
| Chest wall retraction | None | Mild | Moderate | Severe | ||
| Stridor | None | With agitation | At rest | |||
| Cyanosis | None | With agitation | At rest | |||
| Level of consciousness | Normal | Disoriented | ||||
| Air entry | Normal | Decreased | Markedly decreased | |||
Assessment
- <2 Very mild
- 2-6 Mild to moderately severe
- 7-11 Severe croup
- ≥ 12 Respiratory failure
Management
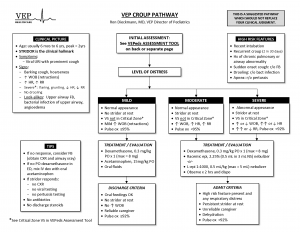
VEP Croup Care Pathway
- Cool mist
- Humidified air may provide symptomatic treatment for patients with ongoing stridor[6]
- Steroids (first line treatment)
- Dexamethasone 0.15-0.6mg/kg PO/IM (max 10mg)[7][8]
- No differences between intramuscular and oral dexamethasone [9]
- Onset 6 hrs, duration 72 hrs
- Recent study showing non-inferiority of low dose (0.15mg/kg) dexamethasone and prednisolone at 1mg/kg[10].
- Epinephrine (nebulized)
- Use in moderate to severe cases based on the croup scores. Use either Racemic or Standard Epinephrine[11]
- Symptomatic relief via local vasoconstriction
- Racemic Epi (2.25%): 0.05 mL per kg (maximal dose: 0.5 mL) of racemic epinephrine 2.25% [12]
- Epinephrine(1:1,000): 0.5 mL per kg (maximal dose: 5 mL) via nebulizer
- Onset up to 30 min, duration 2 hrs
- Watch child 2-3 hrs after administration to ensure no return of stridor at rest
- Intubation
- Rarely needed but if so, use tube that is one half size smaller than normal for age/size of patient
Contraindicated
- Do NOT give albuterol (may worsen edema (vasodilation))
No Evidence
- Heliox
- Mixture of helium and oxygen (with not less than 20% oxygen)
- Low viscosity and low specific gravity facilitates laminar airflow through the respiratory tract.
- Currently there is a lack of evidence to establish the effect of heliox inhalation in the treatment of croup in children[13]
Disposition
Consider Discharge if
- 3hr since last epinephrine
- Able to tolerate PO
- Nontoxic appearance
Admit
- Persistent respiratory symptoms/signs
- ≥2 treatments with epinephrine
Video
START_WIDGET145cf2dedc82b122-0END_WIDGET
See Also
- Bronchiolitis (RSV)
- Prehospital protocol croup
External Links
References
- Rose, E. (2018) Pediatric respiratory emergencies: Upper airway obstruction and infections. Rosen's Emergency Medicine (9th ed.) Philadelphia, PA: Elsevier/Saunders
- Rose, E. (2018) Pediatric respiratory emergencies: Upper airway obstruction and infections. Rosen's Emergency Medicine (9th ed.) Philadelphia, PA: Elsevier/Saunders
- Rose, E. (2018) Pediatric respiratory emergencies: Upper airway obstruction and infections. Rosen's Emergency Medicine (9th ed.) Philadelphia, PA: Elsevier/Saunders
- Westley CR, et al. Nebulized racemic epinephrine by IPPB for the treatment of croup: a double-blind study. Am J Dis Child. 1978; 132(5):484-487.
- Klassen TP, et al. Croup. A current perspective. Pediatr Clin North Am. 1999; 46(6):1167–1178.
- Scolnik D, Coates AL, Stephens D, Da Silva Z, Lavine E, Schuh S. Controlled delivery of high vs low humidity vs mist therapy for croup in emergency departments. JAMA. 2006;295(11):1274–1280
- Geelhoed GC, Macdonald WB. Oral dexamethasone in the treatment of croup: 0.15mg/kg versus 0.3mg/kg versus 0.6mg/kg. Pediatr Pulmonol. 1995;20(6):362–368.
- Bjornson, C.L., Klassen, T.P., Williamson, J., Brant, R., Mitton, C., Plint, A., Bulloch, B., Evered, L. and Johnson, D.W. (2004) ‘A Randomized trial of a single dose of oral dexamethasone for mild Croup’, New England Journal of Medicine, 351(13), pp. 1306–1313.
- Donaldson D, Intramuscular versus oral dexamethasone for the treatment of moderate-to-severe croup: a randomized, double-blind trial. Acad Emerg Med. 2003 Jan;10(1):16-21.
- Prednisolone versus dexamethasone for croup: a randomized controlled trial Parker CM, Cooper MN. Pediatrics. 2019;144(3):e20183772.
- Adair JC, Ring WH, Jordan WS, Elwyn RA. Ten-year experience with IPPB in the treatment of acute laryngotracheobronchitis. Anesth Analg. 1971;50(4):649–55
- Westley CR, Cotton EK, Brooks JG. Nebulized racemic epinephrine by IPPB for the treatment of croup: a double-blind study. Am J Dis Child. 1978;132(5):484–487
- Moraa I, Sturman N, McGuire T, van Driel ML., Heliox for croup in children., Cochrane Database Syst Rev. 2013 Dec 7;12:CD00682
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.