Capitellum fracture
Background
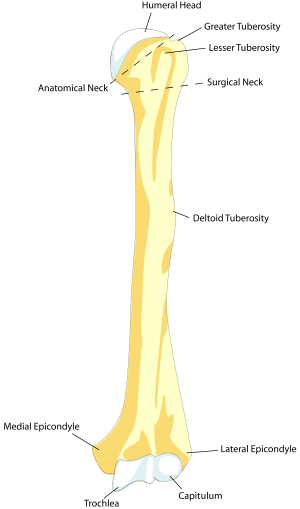
Humeral anatomy
- Fracture of distal humerus at capitellum
- Rare, occurs in approximately 1% of elbow fractures
- Mechanism: FOOSH
- Often require surgery, with good prognosis
Clinical Features
- Pain, swelling, may have block to flexion / extension
Differential Diagnosis
Radiograph-Positive
- Distal humerus fracture
- Radial head fracture
- Capitellum fracture
- Olecranon fracture
- Elbow dislocation
Radiograph-Negative
- Lateral epicondylitis
- Medial epicondylitis
- Olecranon bursitis (nonseptic)
- Septic bursitis
- Biceps tendon rupture/dislocation
Evaluation
- Elbow X-ray
- Fractures are often subtle
- Best seen on lateral XR
- Look for abnormal fat pad
- Look for radiocapitellar line disruption
- If possible, lateral elbow is shot at 45 degrees to pick up subtle fractures
- Consider CT to further identify fracture / operative planning
Management
General Fracture Management
- Acute pain management
- Open fractures require immediate IV antibiotics and urgent surgical washout
- Neurovascular compromise from fracture requires emergent reduction and/or orthopedic intervention
- Consider risk for compartment syndrome
Immobilization
- Long arm posterior splint for Operative / Non operative
Disposition
- Normally outpatient, unless concerning neurovascular injury, open fracture, or coexisting injuries requiring admission
Specialty Outpatient Care
Non-operative management
- Less than 2mm of displacement
Operative management
- More than 2 mm of displacement
- Capitellum with co-existing trochlea involvement
- Comminuted fracture
Potential Complications
- Elbow contracture
- Nonunion
- AVN
- Ulnar nerve injury
References
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.