Clostridium difficile
This page is for adult patients; for pediatric patients see clostridium difficile (peds).
Background

Pseudomembranous colitis with yellow pseudomembranes seen on the wall of the sigmoid colon.
- Clostridium is a genus of gram-positive bacteria
- Most common cause of infectious diarrhea in hospitalized patients
- Use contact isolation if suspect
- Alcohol-based hand sanitizers do not reduce spores, but good hand washing does[1]
Risk factors for Pseudomembranous Colitis
- Recent antibiotic use (any)
- GI surgery
- Severe underlying medical illness
- Chemo
- Elderly
Clinical Features
Varies according to severity and intrinsic host factors (immunosuppression, etc.).
- Profuse watery diarrhea
- Usually develops after 7-10 days of antibiotics use or within 2 weeks of discontinuation
- History of risk factor(s) (see Background)
- May report diffuse abdominal pain/cramping
- At the extreme, may present with sepsis secondary to intestinal perforation or toxic megacolon
Differential Diagnosis
Infectious
- Viral (e.g. rotavirus)
- Bacterial
- Campylobacter
- Shigella
- Salmonella (non-typhi)
- Escherichia coli
- E. coli 0157:H7
- Yersinia enterocolitica
- Vibrio cholerae
- Clostridium difficile
- Parasitic
- Toxin
Noninfectious
- GI Bleed
- Appendicitis
- Mesenteric Ischemia
- Diverticulitis
- Adrenal Crisis
- Thyroid Storm
- Toxicologic exposures
- Antibiotic or drug-associated
Watery Diarrhea
- Enterotoxigenic E. coli (most common cause of watery diarrhea)[2]
- Norovirus (often has prominent vomiting)
- Campylobacter
- Non-typhoidal Salmonella
- Enteroaggregative E. coli (EAEC)
- Enterotoxigenic Bacteroides fragilis
Evaluation
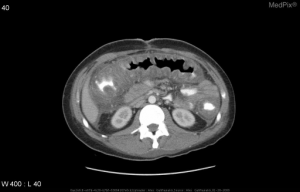
Pseudomembranous colitis from C. difficile on abdominal CT demonstratin diffuse colonic wall thickening and a shaggy endoluminal contour.
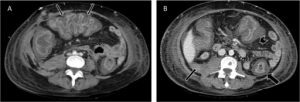
Pseudomembranous colitis with (A) Accordion sign in transverse colon (thin arrows). (B) Colonic wall thickness, target sign (thick arrow), peritoneal fluid (thin arrow) and pericolonic fat stranding (arrowhead).
Workup
- Consider testing patients with unexplained and new-onset ≥3 unformed stools within 24 hours[3]
- Institutions should have an agreed protocol using a stool toxin test as part of a multistep algorithm (e.g. glutamate dehydrogenase [GDH] plus toxin; GDH plus toxin, arbitrated by nucleic acid amplification test [NAAT])
- or NAAT plus toxin) rather than a NAAT alone for all specimens received in the clinical laboratory when there are no preagreed institutional criteria for patient stool submission (Figure 2) (weak recommendation, low quality of evidence).
- C. diff toxin assay
- Sn 63-94%, Sp 75-100%
- Culture
- Positive culture only means C. diff present, not necessarily that it is causing disease
Testing Algorithm
For patients with suspected Clostridium difficile associated diarrhea (CDAD)
- Low suspicion
- Send stool for C. diff toxin assay
- Positive → treat (no further testing indicated)
- Negative → do not treat (no further testing indicated)
- Send stool for C. diff toxin assay
- High suspicion
- Send stool for C. diff toxin assay AND treat empirically
- Positive → treat (no further testing indicated)
- Negative → Consider discussion with ID (false negative tests may occur); eval for other causes of diarrhea
- Send stool for C. diff toxin assay AND treat empirically
Repeat testing
- Never a need for repeat testing within 7 days of a previous test
- NO NEED to repeat positive tests as symptoms resolve as a “test of cure”
- NO NEED to repeat test soon after initial negative test (more likely to be a false positive test than a true positive test)
Severe Criteria[4][5]
- Serum lactate levels >2.2 mmol/l
- Hypotension with or without required use of vasopressors
- Ileus or significant abdominal distention
- Mental status changes
- WBC ≥35,000 cells/mm3 or <2,000 cells/mm3
- Patient requiring ICU admission
- End organ failure (mechanical ventilation, renal failure, etc.)
Management
Asymptomatic
- No diagnostic testing or treatment required[6]
Mild
- Either discontinue offending antibiotics (if possible) or give metronidazole 500mg PO q6hr x10-14d
Moderate
- Vancomycin 125 mg PO four times daily
- Fidaxomicin 200 mg PO two times daily
- Metronidazole 500mg PO or IV q6hr x10-14d (third line therapy)
Severe
See criteria above (Evaluation section)
- Vancomycin 125-250mg PO q6hr x10d (IV form is not effective)
- Add Metronidazole 500mg IV q6hr if ileus or patient cannot tolerate PO
- Consider emergency colectomy if:
- WBC >20K
- Lactate >5
- Age >75
- Immunosuppression
- Toxic megacolon
- Colonic perforation
- Multi-organ system failure
Recurrent Infection
Relapse occurs in 10-25% of patients
- Occurs <=4 weeks after the completion of therapy
- Otherwise consider other (more common) causes
- 1st recurrence: same agent as used to treat initial episode (antimicrobial resistance is not clinically problematic)
- 2nd recurrence: tapered vancomycin with pulse doses
- 3rd recurrence: PO vancomycin 10-14 days followed immediately by rifaximin "chaser" 400mg TID x20 days [7]
- Other options:
- IVIG
- Fecal transplant
- Fidaxomicin 200mg BID x10 days noninferior to PO vancomycin, and reduces recurrences at 4 weeks after treatment (~15% vs 25%) [8]
Disposition
- Admit:
- Severe diarrhea
- Outpatient antibiotic failure
- Systemic response (fever, leukocytosis, severe abdominal pain)
Antibiotic Sensitivities[9]
See Also
References
- Leffler DA and Lamont JT. Clostridium difficile Infection. N Engl J Med. 2015; 372:1539-1548.
- Marx et al. “Cholera and Gastroenteritis caused by Noncholera Vibrio Species”. Rosen’s Emergency Medicine 8th edition vol 1 pg 1245-1246.
- Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA) McDonald CL, et al. Clinical Infectious Diseases, Volume 66, Issue 7, 1 April 2018, Pages e1–e48, https://doi.org/10.1093/cid/cix1085
- IDSA Guidelines PDF
- ACG Guidelines for Diagnosis, Treatment, and Prevention of Clostridium difficile Infections http://gi.org/guideline/diagnosis-and-management-of-c-difficile-associated-diarrhea-and-colitis/
- Bagdasarian, N, et al. Diagnosis and Treatment of Clostridium difficile in Adults. JAMA. 2015; 313(4):398-408.
- Melville NA. Rifaximin 'Chaser' Reduces C difficile Recurrent Diarrhea. June 07, 2011. http://www.medscape.com/viewarticle/744157
- Louie TJ et al. Fidaxomicin versus Vancomycin for Clostridium difficile Infection. N Engl J Med 2011; 364:422-431.
- Sanford Guide to Antimicrobial Therapy 2014
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.