Brown-Séquard syndrome
Background
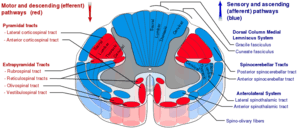
Spinal cord tracts
- Transverse hemisection of spinal cord
- Unilateral cord compression
Clinical Features
- Decussation of corticospinal tract at the medulla and complete lack of decussation of fibers of the posterior columns result in:
- Ipsilateral spastic paresis
- Ipsilateral loss of proprioception, vibration
- Decussation of anterolateral fibers within spinal tract one level up via anterior white commissure results in:
- Contralateral loss of pain, temperature (ie 'sensory dissociation')
Differential Diagnosis
Spinal Cord Syndromes
Evaluation
- Clinical presentation and mechanism
Management
- Consider intubation injuries at C5 or above
- Consider surgical intervention for:
- Progressive neurologic deficits
- Unstable spine fractures
- Steroids are no longer recommended
Administration of methylprednisolone (MP) for the treatment of acute spinal cord injury (SCI) is not recommended. Clinicians considering MP therapy should bear in mind that the drug is not Food and Drug Administration (FDA) approved for this application. There is no Class I or Class II medical evidence supporting the clinical benefit of MP in the treatment of acute SCI. Scattered reports of Class III evidence claim inconsistent effects likely related to random chance or selection bias. However, Class I, II, and III evidence exists that high-dose steroids are associated with harmful side effects including death.
[1]- See EBQ:High Dose Steroids in Cord Injury for further discussion
Prognosis
- Good
Disposition
- Admission
See Also
- Spinal cord syndromes
External Links
References
- Hurlbert RJ et al. Pharmacological therapy for acute spinal cord injury. Neurosurgery. 2013 Mar;72 Suppl 2:93-105 http://www.ncbi.nlm.nih.gov/pubmed/23417182
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.