Symptomatic cholelithiasis
Background
Anatomy & Pathophysiology
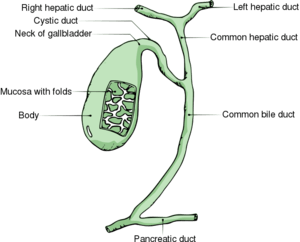
Gallbladder anatomy
- Gallstones are classified as cholesterol stones and pigmented stones (black and brown), and are present in approx 20% of females and 8% of males in the United States
- These stones cause the majority of all biliary tract problems, and depending on where the stone become impacted, specific problems occur.
- Bile flows out the gallbladder, down the cystic duct into the common bile duct, and ultimately into the 1st portion of the duodenum.
Gallbladder disease types
- Acute calculous cholecystitis
- Cholangitis (ascending cholangitis)
- Symptomatic cholelithiasis (biliary colic)
- Acalculous cholecystitis
- Choledocholithiasis
Clinical Features
History
- RUQ pain that is constant, lasts 1-5hr, and then remits
- Pain >5hr suggests cholecystitis, cholangitis, or pancreatitis
- Usually does not occur during fasting
- Radiation to the right shoulder increases likelihood, but is not sensitive
Physical Exam
- Often benign; as compared to cholecystitis, usually negative Murphy's Sign
Differential Diagnosis
RUQ Pain
- Gallbladder disease
- Peptic ulcer disease with or without perforation
- Pancreatitis
- Acute hepatitis
- Pyelonephritis
- Pneumonia
- Kidney stone
- Pancreatitis
- GERD
- Appendicitis (retrocecal)
- Pyogenic liver abscess
- Fitz-Hugh-Curtis Syndrome
- Hepatomegaly due to CHF
- Herpes zoster
- Myocardial ischemia
- Bowel obstruction
- Pulmonary embolism
- Abdominal aortic aneurysm
Evaluation
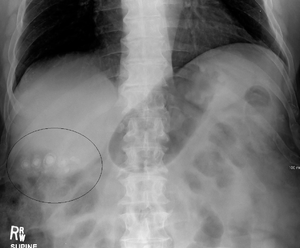
Gallstones found incidentally on KUB (xrays are not sensitive).
- Labs
- LFTs, CBC normal
- RUQ Ultrasound
- Sensitivity 84%, Specificity 99%
Disposition
- Discharge
References
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.