Arterial gas embolism
Background
- Also known as "air embolism"
- May be fatal when air entry reaches 200-300 mL (pressure gradient of 5 mmHg across 14 ga catheter entrains air at 100 mL/sec)[1]
- Dialysis related
- Due to negative intrathoracic pressure from spontaneous breathing
- Scuba related
- Results from pulmonary barotrauma (most common) and decompression sickness
Prevention
- Positive pressure mechanical ventilation reduces positive pressure gradient
- Trendelenburg for insertion/removal of IJV and subclav lines
- Reverse Trendelenburg for femoral
Clinical Features
- Asymptomatic
- Mild: dyspnea, cough
- Cardiogenic shock: hypotension, oliguria, altered mental status, chest pain
- Dialysis related
- Acute dyspnea, chest tightness, LOC, cardiac arrest, arrhythmia[2]
- Scuba related
- Symptoms develop during ascent or immediately upon surfacing
- Causes variety of stroke syndromes depending on part of brain affected
- Immediate death, loss of consciousness, seizure, blindness, hemiplegia
Differential Diagnosis
Dialysis Complications
- Dialysis-associated hypotension
- Dialysis disequilibrium syndrome
- Air embolism
- Missed dialysis (pulmonary edema)
Scuba Diving Emergencies
- Barotrauma of descent
- Otic barotrauma
- Sinus barotrauma
- Face squeeze
- Barotrauma of ascent
- At depth injuries
- Oxygen toxicity
- Nitrogen narcosis
- Hypothermia
- Contaminated gas mixture (e.g. CO toxicity)
- Caustic cocktail from rebreathing circuit
Evaluation
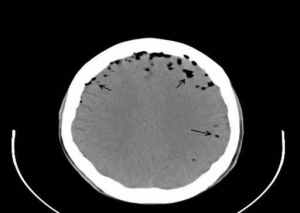
Cerebral air embolism with multiple air bubbles.
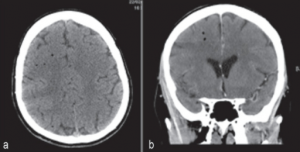
Fatal cerebral arterial gas embolism. (a) CT head showing air bubbles predominantly in the right cerebral hemisphere (b) CT head showing air bubbles predominantly in the right cerebral hemisphere
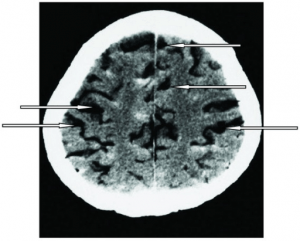
Arterial air embolism (arrows)
- Low ETCO2 in significant venous air embolism
- TEE: most sensitive, invasive not available in emergencies
- Doppler US: noninvasive; air in chamber = high pitch sound
Management[3][4]
- Central line aspiration of air from right heart
- 100% O2 non-rebreather
- Regardless of SaO2 (to reduce embolism size)
- Hemodynamic support with positive inotropes
- CPR in large air embolus
- Positioning
- Durant's maneuver - left lateral decubitus and Trendelenburg
- Traps air in apex of RV, relieves obstruction of pulmonary outflow tract
- May require open surgical or angiography for recovery of residual intracardiac or intrapulmonary air
Dialysis Related
- Prevent any further air entry
- Immediately cover puncture site with saline soaked gauze
Scuba Related
- IVF (increases tissue perfusion)
- Rapid recompression
Disposition
- Likely admission
External Links
References
- Vascular Access. In: Marino, P. The ICU Book. 4th, North American Edition. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2013
- Diving Medicine, Karen B. Van Hoesen and Michael A. Lang, Auerbach's Wilderness Medicine, Chapter 71, 1583-1618.e6
-
- Shaikh N., Ummunisa F. Acute management of vascular air embolism. J Emerg Trauma Shock. 2009 Sep-Dec; 2(3): 180–185.
- Gordy S and Rowell S. Vascular air embolism. Int J Crit Illn Inj Sci. 2013 Jan-Mar; 3(1): 73–76.
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.