Antipsychotic toxicity
Background
- Isolated overdose of antipsychotics is rarely fatal
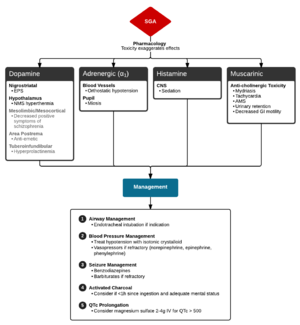
- Toxicity results in blockade of some or all of the following receptors:
- Dopamine - extrapyramidal symptoms
- α-1 - orthostatic hypotension, reflex tachycardia
- Muscarinic - anticholinergic symptoms
- Histamine - sedation
Clinical Features
Evaluation of SGA (Second Generation Antipsychotic) Toxicity
- Extrapyramidal
- Acute dystonic reaction
- Tongue protrusion, facial grimacing, trismus, oculogyric crisis
- Akathisia
- Acute dystonic reaction
- CNS
- Lethargy, ataxia, dyarthria, confusion, coma
- Seizure (1%)
- Anticholinergic Effects
- Tachycardia, dry mucous membranes, dry skin, decreased bowel sounds, delirium
- ECG changes
- Sinus tachycardia
- QT prolongation
Differential Diagnosis
Anticholinergic toxicity Causes
- Medications
- Atropine
- Antihistamines
- Antidepressants
- Tricyclic antidepressant (TCA) toxicity
- SSRIs
- Antipsychotics
- Muscle relaxants
- Anti-Parkinsonians
- Plants
- Jimson weed (Devil's trumpet)
- Amanita mushroom
Evaluation
Workup
- POC Glucose
- ECG (QT interval)
- Co-ingestions: serum acetaminophen, salicylate, EtOH level, other known drug levels
- Urine toxicology screen
- Chemistry (metabolic acidosis, electrolytes, renal function)
- LFT (hepatotoxicity)
- CK (rhabdomyolysis)
- Serum osmolarity (osmolar gap)
- ABG (carboxyhemoglobin, methemoglobin)
Management
Supportive
- Hypotension
- QT prolongation
- Treat all with QTc >500ms with magnesium 2-4gm IV over 10min
Extrapyramidal
- Diphenhydramine 25-50mg IV/IM OR benztropine 1-2mg IV/IM
- Oral therapy with either of above meds should be continued for 2 weeks
Disposition
- Consider discharge after 6hr as long as there are all of the following:
- No mental status changes
- Normal HR/BP
- No orthostatic hypotension
- Normal QT interval
See Also
External Links
References
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.