Anterior cord syndrome
Background
- Etiology
- Direct anterior Cord Compression (e.g. disc protrusion, posterior abdominal aortic aneurysm, mass)
- Hyperflexion injury of cervical spine
- Thrombosis of anterior spinal artery
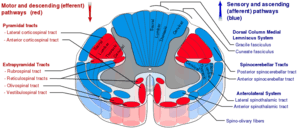
Spinal cord tracts
Clinical Features
- Paraplegia below level of lesion (corticospinal)
- Loss of pain/temperature (lateral spinothalamic)
- Autonomic dysfunction, orthostasis
- Bowel, bladder, sexual dysfunction
- Preservation of modalities carried by dorsal columns i.e. vibration, proprioception, 2-point discrimination
Differential Diagnosis
Spinal Cord Syndromes
- Complete spinal cord transection syndrome
- Anterior cord syndrome
- Central cord syndrome
- Brown-Sequard syndrome
- Epidural compression syndromes
- Etiologies
- Trauma, vertebral fractures
- Ischemia, atherosclerosis, anterior spinal artery
- Malignancy
- Infection
- Spondylosis, disk herniation
- Aortic disease - aneurysm, dissection
- Iatrogenic - spinal injections, epidural catheters, aortic cross-clamp
Evaluation
- Labs based on severity
- ABG if lesion affects above C5
- Shock labs if neurogenic shock
- Trend CBC to rule out hemorrhagic shock
- Imaging with CT and MRI
Management
- Consider intubation injuries at C5 or above
- Consider surgical intervention for:
- Progressive neurologic deficits
- Unstable spine fractures
- Steroids are no longer recommended
Administration of methylprednisolone (MP) for the treatment of acute spinal cord injury (SCI) is not recommended. Clinicians considering MP therapy should bear in mind that the drug is not Food and Drug Administration (FDA) approved for this application. There is no Class I or Class II medical evidence supporting the clinical benefit of MP in the treatment of acute SCI. Scattered reports of Class III evidence claim inconsistent effects likely related to random chance or selection bias. However, Class I, II, and III evidence exists that high-dose steroids are associated with harmful side effects including death.
[1]- See EBQ:High Dose Steroids in Cord Injury for further discussion
- Neurogenic shock management
Prognosis
- Poor
Disposition
- Admit
External Links
See Also
- Spinal cord syndromes
References
- Hurlbert RJ et al. Pharmacological therapy for acute spinal cord injury. Neurosurgery. 2013 Mar;72 Suppl 2:93-105 http://www.ncbi.nlm.nih.gov/pubmed/23417182
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.