Acalculous cholecystitis
Background
- Acute necroinflammatory disease of gallbladder with multifactorial pathogenesis
- Gallbladder stasis and ischemia leads to distension and eventually necrosis/perforation
- Accounts for 10% of acute cholecystitis; associated with high morbidity/mortality
Anatomy & Pathophysiology
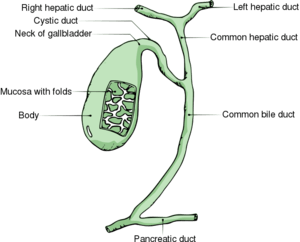
Gallbladder anatomy
- Gallstones are classified as cholesterol stones and pigmented stones (black and brown), and are present in approx 20% of females and 8% of males in the United States
- These stones cause the majority of all biliary tract problems, and depending on where the stone become impacted, specific problems occur.
- Bile flows out the gallbladder, down the cystic duct into the common bile duct, and ultimately into the 1st portion of the duodenum.
Gallbladder disease types
- Acute calculous cholecystitis
- Cholangitis (ascending cholangitis)
- Symptomatic cholelithiasis (biliary colic)
- Acalculous cholecystitis
- Choledocholithiasis
Risk Factors
- Burns
- CAD
- DM
- Immunosuppression
- Infection
- Mechanical ventilation
- Medications (eg, opioids, sunitinib)
- Multiple transfusions
- Nonbiliary surgery
- Sepsis/hypotension
- Vasculitis
- TPN, especially TPN > 3 mo
Clinical Features
- Similar to calculous cholecystitis
- Jaundice is common (20% of patients)
Differential Diagnosis
RUQ Pain
- Gallbladder disease
- Peptic ulcer disease with or without perforation
- Pancreatitis
- Acute hepatitis
- Pyelonephritis
- Pneumonia
- Kidney stone
- Pancreatitis
- GERD
- Appendicitis (retrocecal)
- Pyogenic liver abscess
- Fitz-Hugh-Curtis Syndrome
- Hepatomegaly due to CHF
- Herpes zoster
- Myocardial ischemia
- Bowel obstruction
- Pulmonary embolism
- Abdominal aortic aneurysm
Evaluation
Work-Up
- CBC
- Leukocytosis (70-85% of patients)
- Chemistry
- LFTs
- Hyperbilirubinemia
- Alk phos elevation (mild)
- Transaminitis
- Blood cultures
- RUQ Ultrasound
- Absence of gallstones or sludge
- Thickened wall (>5 mm) with pericholecystic fluid
- Positive sonographic Murphy's sign
- Emphysematous cholecystitis with gas bubbles arising in fundus of gallbladder
- Frank perforation of gallbladder with associated abscess formation
Management
- Antibiotics
- Cholecystectomy
- Definitive therapy
Disposition
- Admit
See Also
References
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.