Acute abdominal series
Technique
3 Films:
- Upright chest film
- Rule-out free air
- Upright abdominal film
- Look for air-fluid levels
- Supine abdominal film (KUB = just supine film)
- Width of bowel loops most visible (estimate of amount of distention)
If patient does not tolerate upright position, left lateral decubitus abdominal film can substitute
Interpretation
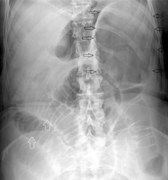
 Normal
Normal
 Large bowel obstruction (Cecal volvulus; black arrows).
Large bowel obstruction (Cecal volvulus; black arrows).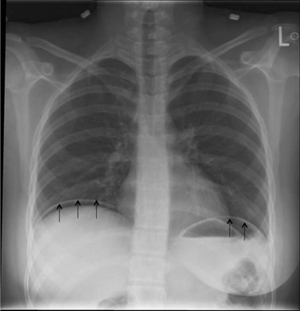 Free intra-abdominal air below the diaphragm.
Free intra-abdominal air below the diaphragm.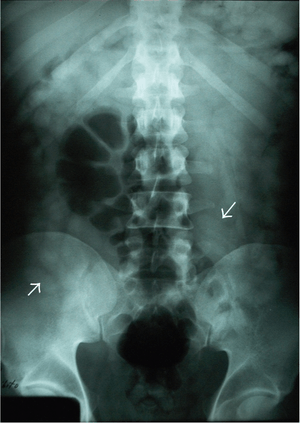 Body-packing with multiple foreign bodies ("balls" of hashish).
Body-packing with multiple foreign bodies ("balls" of hashish).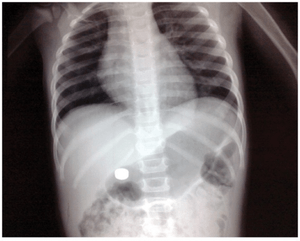
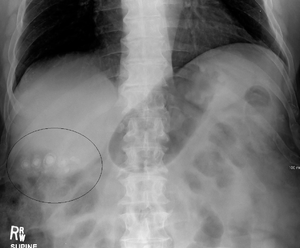 Gallstones (not sensitive)
Gallstones (not sensitive)

Differentiating large and small bowel
| Location | Size | Lines |
| Small bowel | 3 cm | All the way through the bowel (plica circulares) |
| Colon | 6 cm | Only halfway through the bowel (haustra) |
| Cecum | 9 cm |
Small bowel obstruction
- Air in colon or rectum makes complete obstruction less likely (esp if symptoms >24hr)
- Abdominal x-ray has poor Sn and Sp for SBO
- If concerned need CT
Indications
- Ruling out free air under the diaphragm (e.g. perforated ulcer)
- Ruling out radio-opaque abdominal foreign body (e.g. swallowed battery)
- Ruling in bowel obstruction (i.e. to avoid need for subsequent CT scan)
- Do NOT use as the sole study to rule out bowel obstruction (poor sensitivity)
- Do NOT use to rule out generalized peritonitis (almost no sensitivity for diagnoses such as appendicitis)
- Do NOT use to diagnose constipation (many patient with acute abdomen will have "copious stool")
Incidental findings
- Gallstones (not always radiodense)
See Also
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.