25C-NBOMe
Although this article specifically addresses 25C-NBOMe, there are also 25I- and 25B- versions of the compound
Background
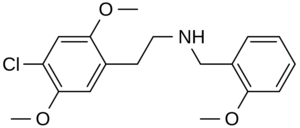
25C-NBOMe

Blotter paper containing 25C-NBOMe
- 2-(4-chloro-2,5-dimethoxyphenyl)-N-[(2-methoxyphenyl)methyl]ethanamine
- Other names: NBOMe-2C-C, Boom, C-Boom, Cimbi-82, Pandora, N-bomb, Holland film, Dime
- Potent partial agonist of 5-HT2A receptor[1]
- First synthesized in Germany by Ralf Heim in 2004[2]
- Member of new class of toxic phenethylamine derivatives (NBOMe) with similar effects to LSD
- Commonly ingested orally or sublingually; can also be taken nasally, parenterally, vaginally, rectally.
- Dose of 50-200 micrograms causes hallucinogenic effects[1]
- Onset 0-15 mins, peak 30-90 mins, total duration 4-10 hours[1]
- Case reports of ingestions have included overdose symptoms of grand mal seizures and purpuric rash and mydriasis with 25B-NBOMe variant[3]
- The 25I- version of the drug has symptoms described as tachycardia, hallucinations, hypertension, and seizures and agitation.[4]
Clinical Features
- Metallic chemical taste
- Sense of numbness of tongue and mouth
- Euphoria
- Visual/Auditory hallucinations
- Stimulation +/- tremors, bruxism
- Serotonin Syndrome (altered mental status, Hyperthermia, rigidity, autonomic instability)[5]
- Confusion
- Agitation
- Vasoconstriction
- Nausea and Vomiting
- Headache
- Palpitations
- Diaphoresis
- Dysuria
- Hypertension
- Generalized Seizure
- Mydriasis
- Acute Renal Failure
- Metabolic Acidosis
Differential Diagnosis
Drugs of abuse
- 25C-NBOMe
- Alcohol
- Amphetamines
- Bath salts
- Cocaine
- Ecstasy
- Gamma hydroxybutyrate (GHB)
- Heroin
- Inhalant abuse
- Hydrocarbon toxicity
- Difluoroethane (electronics duster)
- Marijuana
- Phencyclidine (PCP)
- Psilocybin ("magic mushrooms")
- Synthetic cannabinoids
Evaluation
- Urine pregnancy
- CBC, Metabolic panel, LFTs, coags, APAP level, ASA level
- Total CK level
- ECG
- UA
- Tox screen, blood alcohol
- Serum osmoles, urine Na (if Hyponatremia present)
- Head CT as indicated
- LP to rule out Meningitis if infectious symptoms and based on history and physical
Management
- ABCs
- IV, O2, monitor
- Agitation
- Benzodiazepines
- Haldol for acute agitation
- Seizure
- Hyperthermia:
- Passive cooling measures
Disposition
- Admit for monitoring on all patients with continuing agitation requiring escalating doses of sedation
- Consider discharge if complete resolution of symptoms
References
- Bersani FS, Corazza O, Albano G, et al. 25C-NBOMe: preliminary data on pharmacology, psychoactive effects, and toxicity of a new potent and dangerous hallucinogenic drug. Biomed Res Int. 2014;2014:734749.
- Heim R. “Synthese und Pharmakologie potenter 5-HT2A-Rezeptoragonisten mit N-2-Methoxybenzyl-Partialstruktur”. :Entwicklung eines neuen Struktur-Wirkungskonzepts. Berlin, Freie University, Dissertation, 2003
- Poklis JL. et al. Determination of 4 bromo 2,5 dimethoxy N [2 methoxyphenyl) methyl] benzeneethanamine (25B-NBOMe) in serum and urine by high performance liquid chromatography with tandem mass spectrometry in a case of severe intoxication. Drug Test Anal. 2004;6:764-9
- Poklis J. Devers KG et al. Postmortem detection of 25I-NBOMe [2-(4-iodo-2,5-dimethoxyphenyl)methyl] ethanamine] in fluids and tissues determined by high performance liquid chromatography with tandem mass spectrometry from a traumatic death. Forensic Sci Int. 2014;234:e14-e20
- Boyer EW, Shannon M. The serotonin syndrome. NEJM. 2005;352:1112-20
This article is issued from
Wikem.
The text is licensed under Creative
Commons - Attribution - Sharealike.
Additional terms may apply for the media files.